This post summarizes the results of my analysis of CFSA’s FY2023 data, compared to the data from FY2022 and previous years. Except when otherwise noted, the data is drawn from the Public Dashboard of the District of Columbia’s Child and Family Services Agency (CFSA), which provides data, updated quarterly, on the agency’s essential functions. My analysis showed a large increase in hotline calls in the last year, but a decrease in the number of investigations and substantiated claims of abuse or neglect. The foster care and in-home caseloads continued to fall, with a precipitous drop in the opening of in-home cases in particular. An important finding was the decline since 2019 in the number of in-home and foster case opened as a proportion of substantiated investigations. Taken together, the data suggest an agency that is withdrawing its core mission of responding to abuse and neglect in favor of new initiatives that are more in accord with the current ideological climate in child welfare.
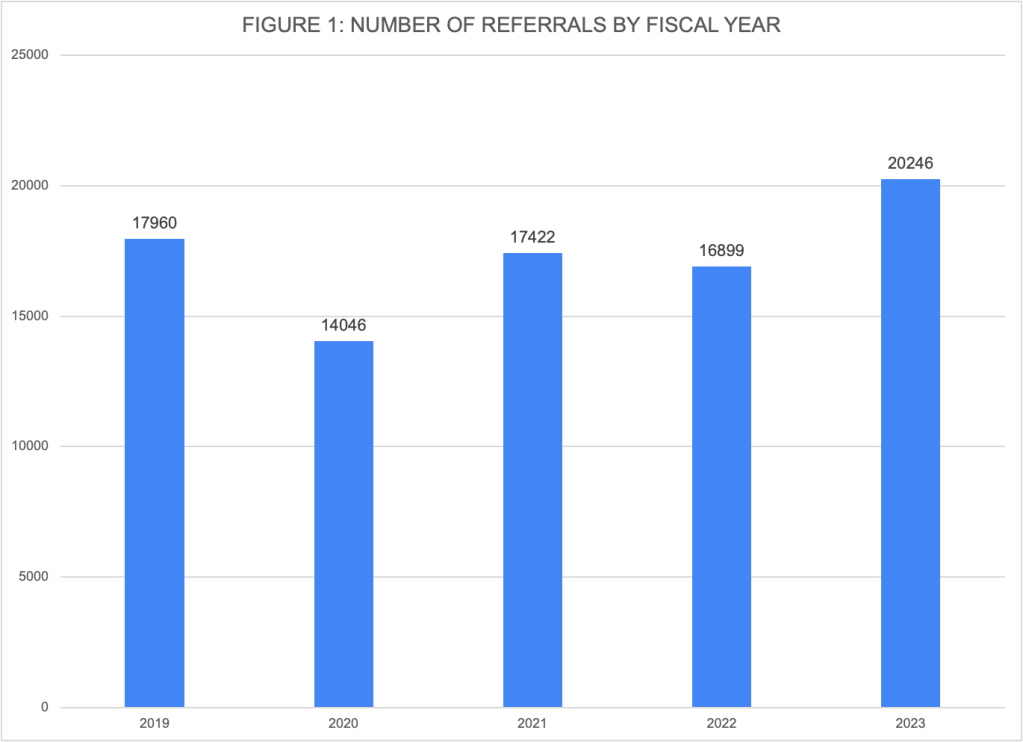
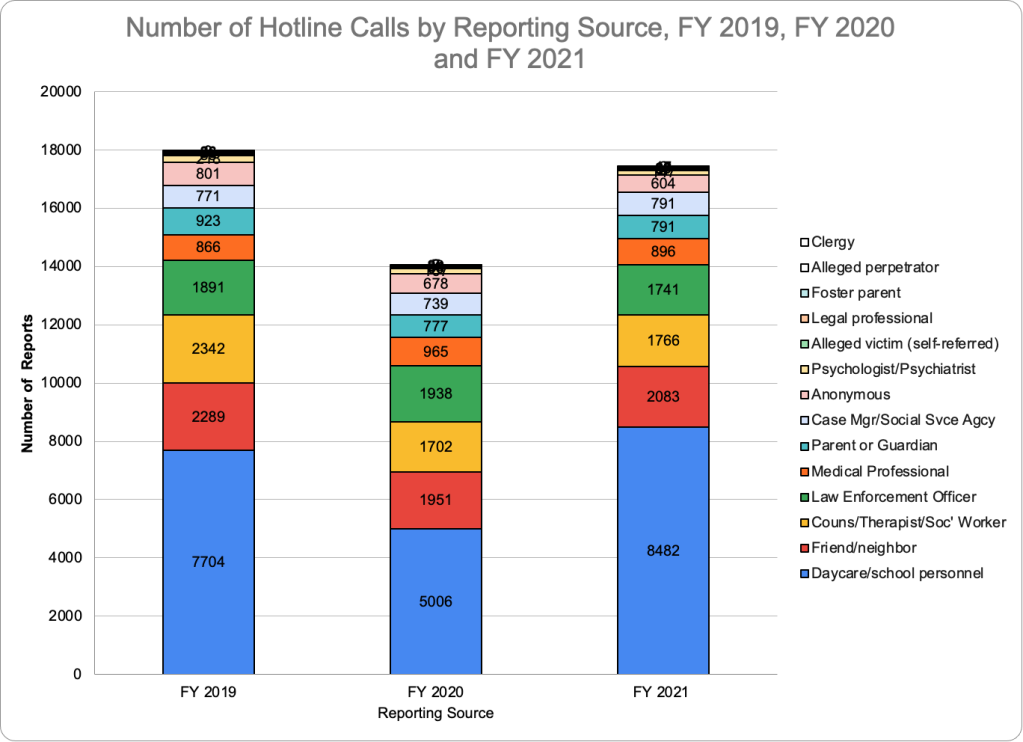
There were 20,246 calls to the CFSA hotline (called “referrals” by the agency) in FY 2023. About 51 percent of the referrals came from school and daycare personnel; that share has increased to more than its pre-pandemic level of 42.9 percent in 2019. Nationally, teachers, made only 20.7 percent of referrals in FY2022. The District’s very different reporting pattern may reflect its educational neglect law, which requires teachers to make a report when a child has more than ten unexcused absences in a year.
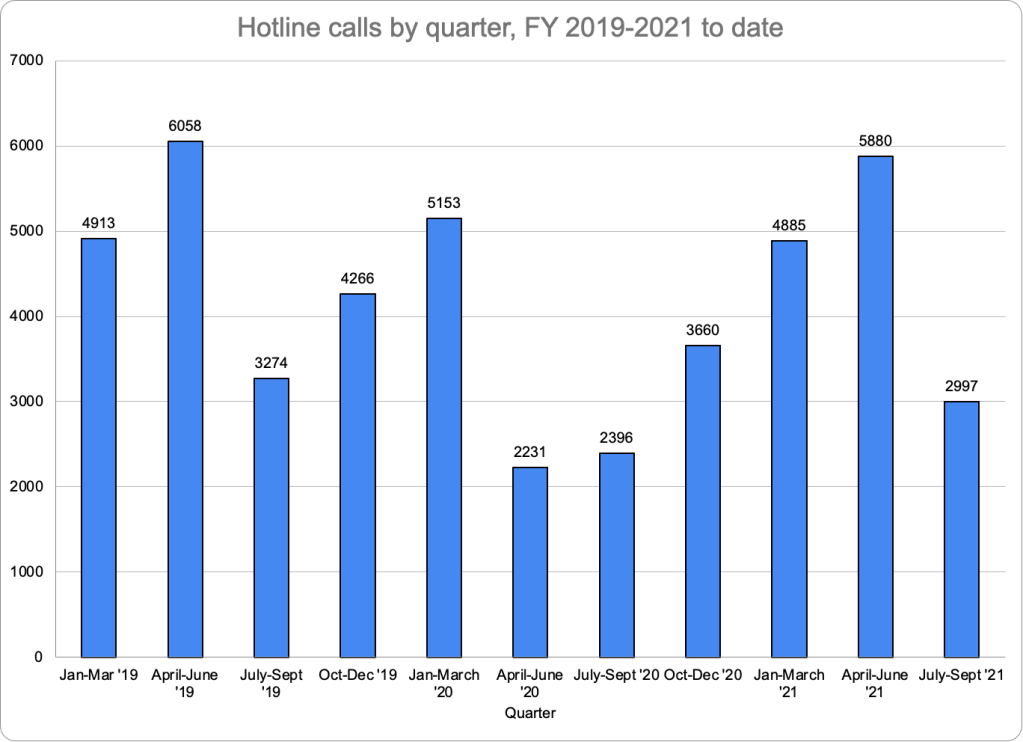
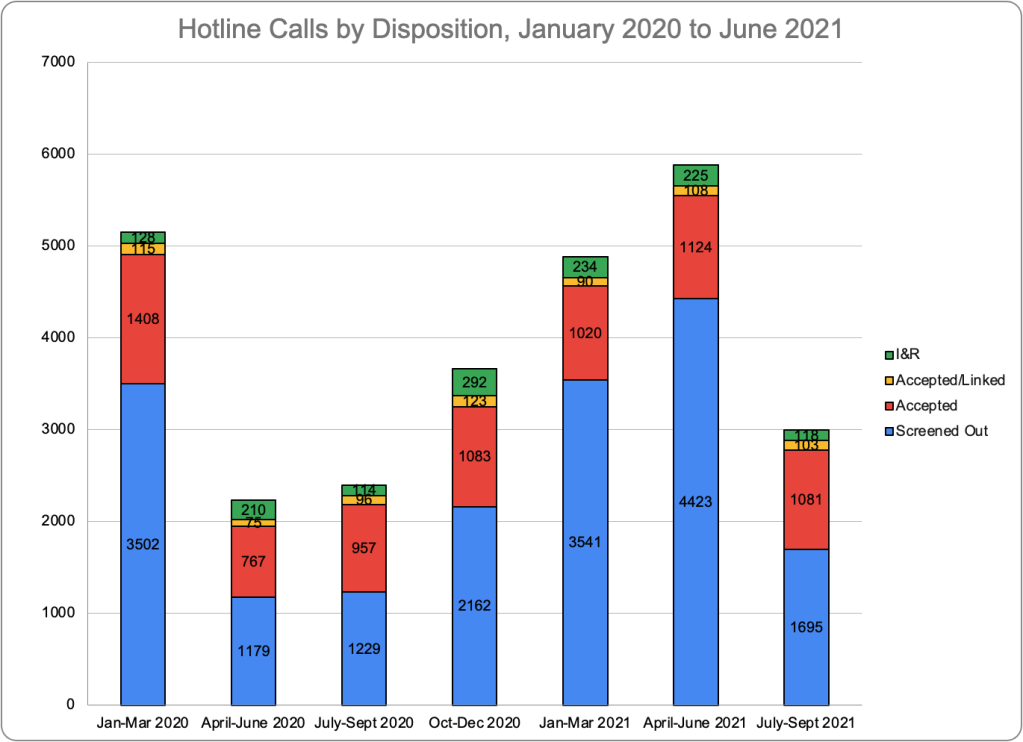
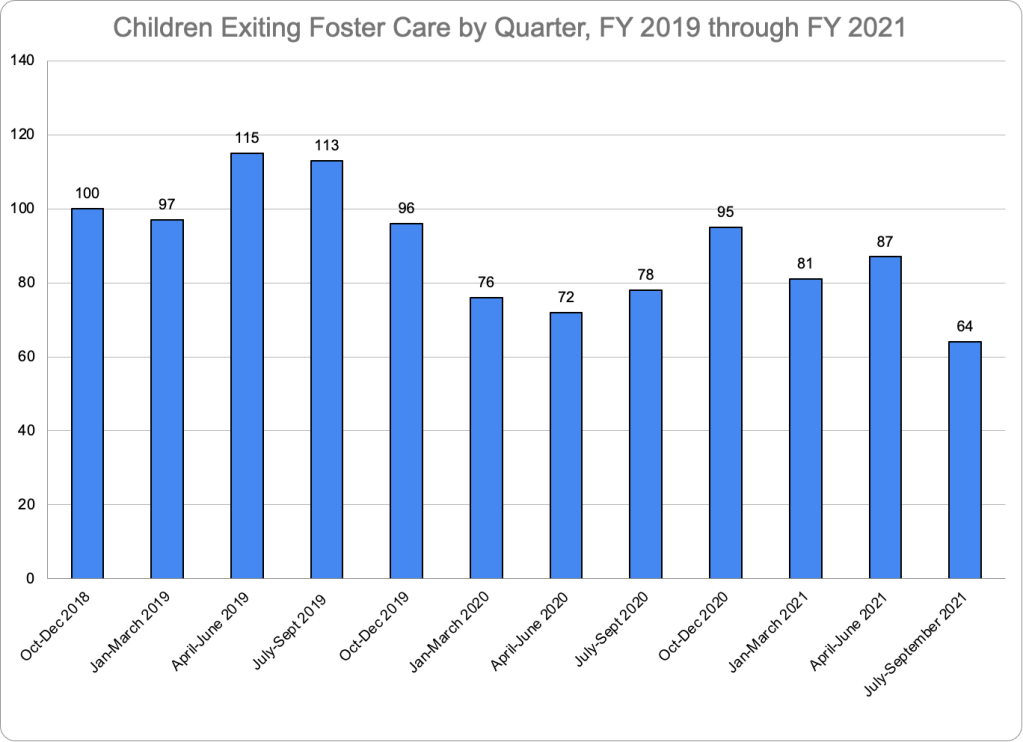
Figure 1 shows the precipitous drop in referrals during the pandemic year of 2020, followed by an increase in FY2021, and a slight dip in FY2022. The total of 20,246 calls to the hotline in FY2023 was 20 percent above the total of 16,899 in FY2022 and even eclipsed that of the year before the pandemic. Most sources increased their reporting in FY2023, but much of the increase came from school and childcare personnel, who made 10,329 reports in FY2023 compared to 8,389 in FY2022. It is not clear why referrals increased so much in FY2023.
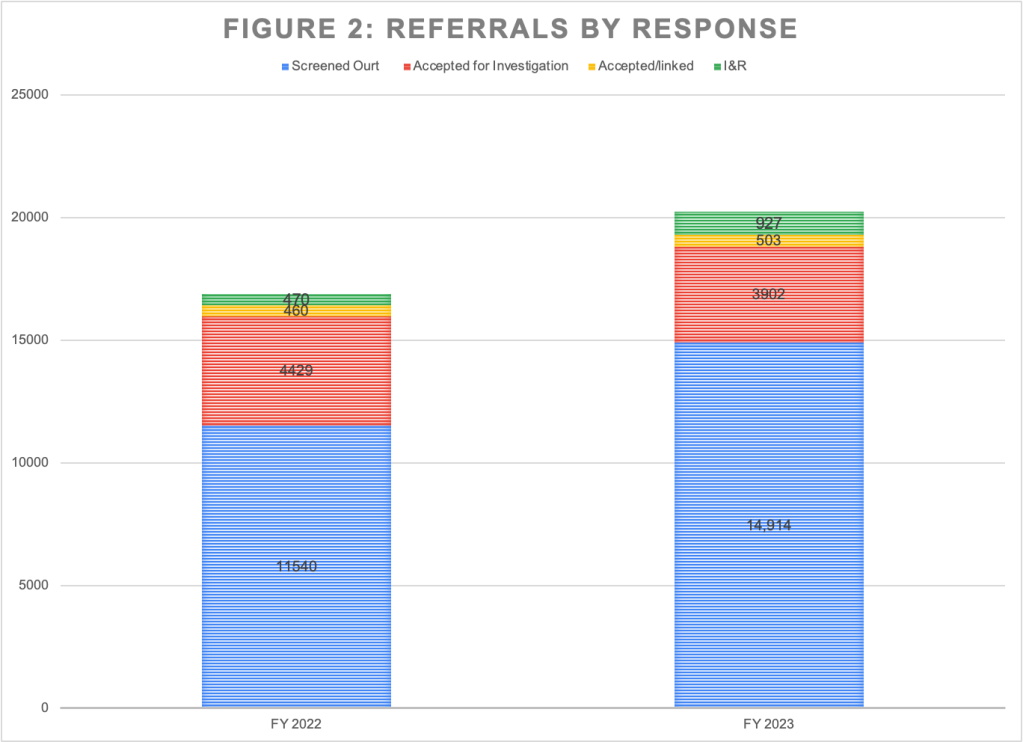
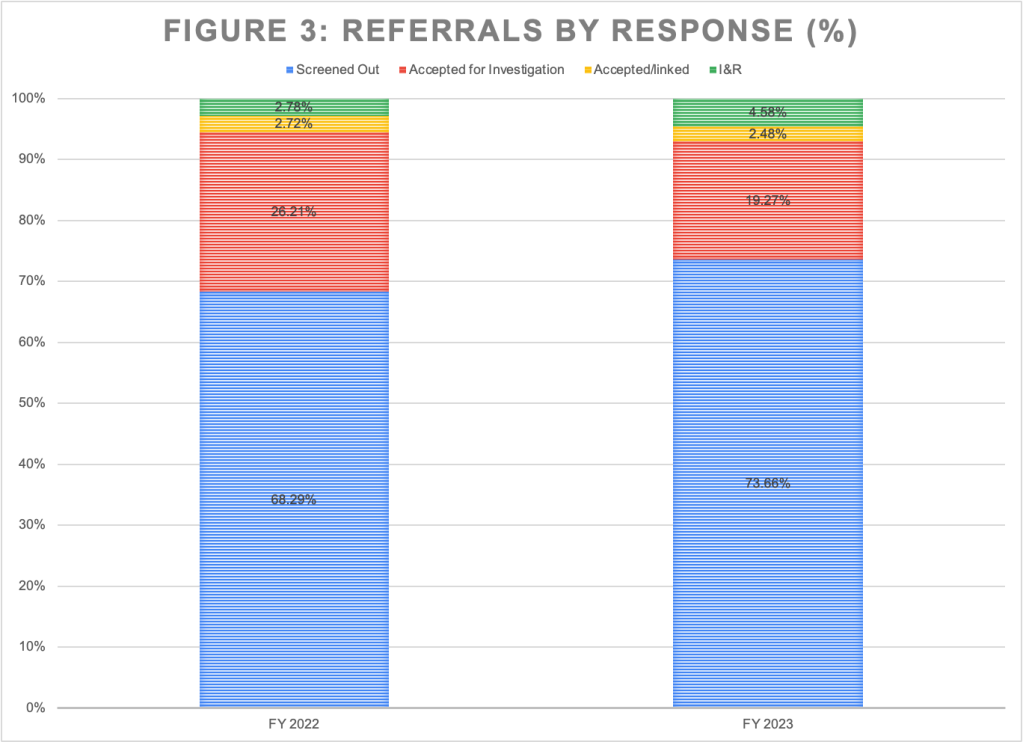
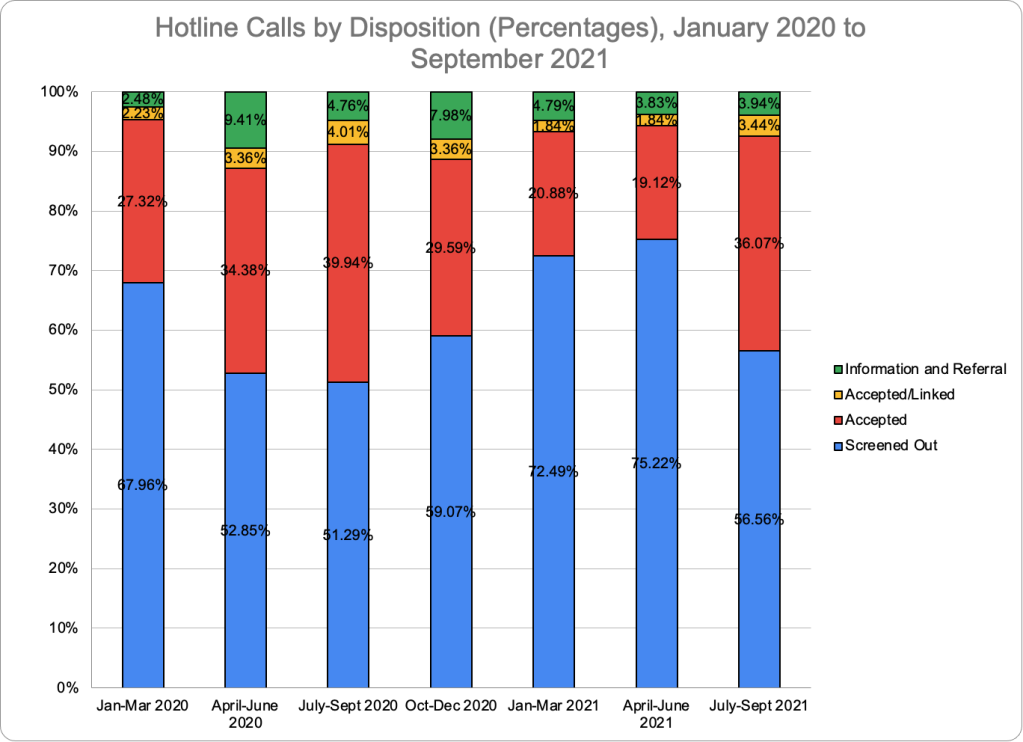
CFSA responded to the increase in referrals by screening out a larger percentage of these calls and accepting a smaller percentage for investigation. Out of the 20,246 referrals received in FY2023, CFSA hotline staff screened out 11,540 or 73.7 percent, compared to the 68.3 percent of referrals they screened out the year before, as shown in Figure 3. And they accepted only 19.3 percent, as compared to the 26.2 percent they accepted the year before. (Referrals not screened out or accepted were linked to an existing investigation or redirected to another agency). Hotline staff actually accepted significantly fewer referrals for investigation in FY2023 than in FY2022 despite the increase in referrals-a total of 3,902 accepted referrals in FY2023 compared to 4,429 the previous year, as FIgure 2 shows.
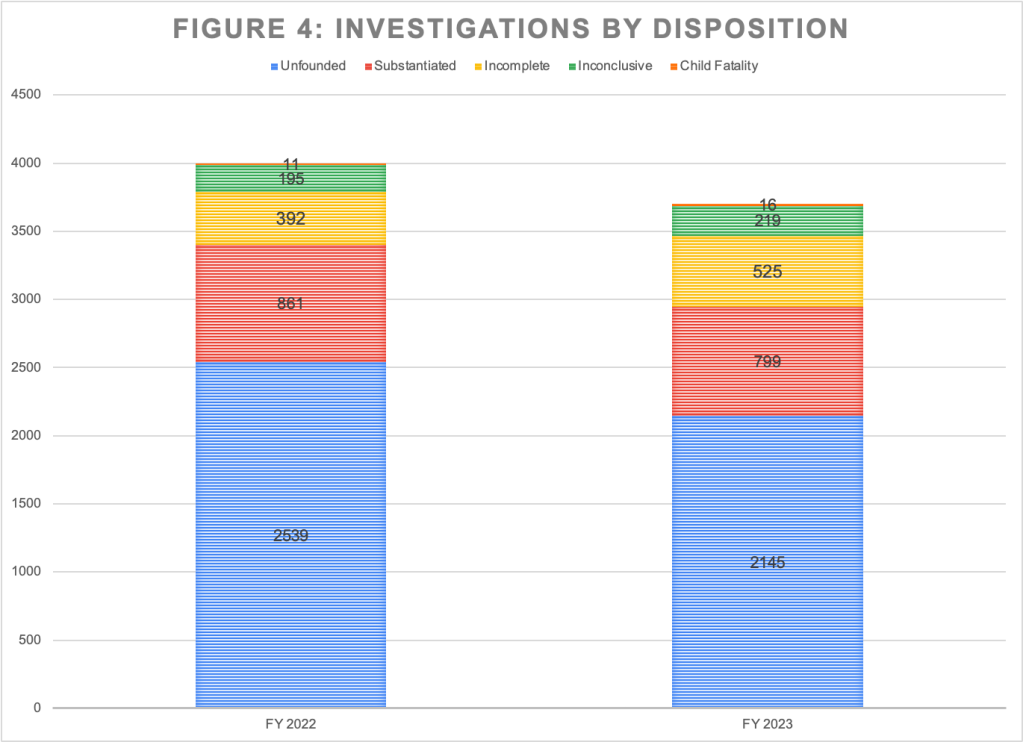
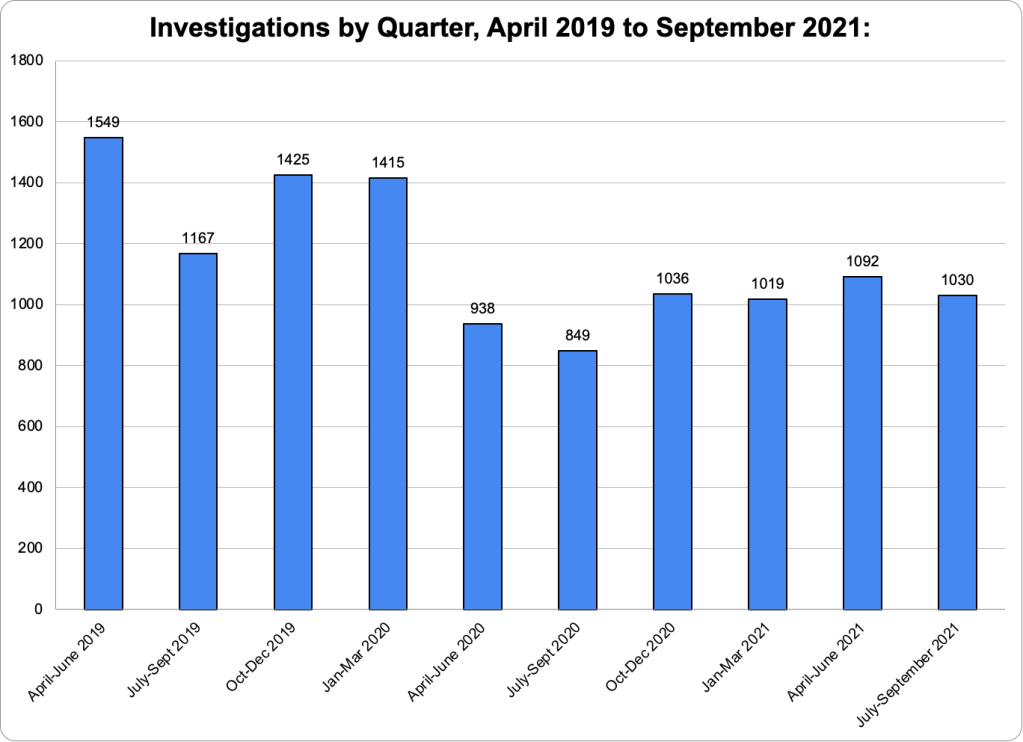
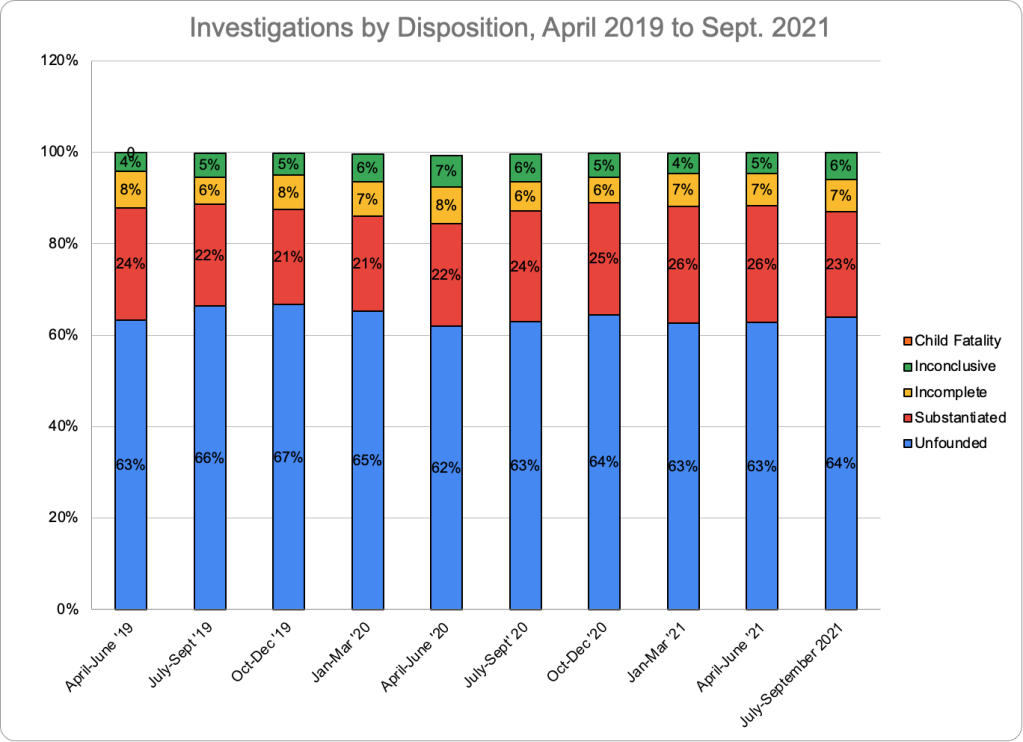
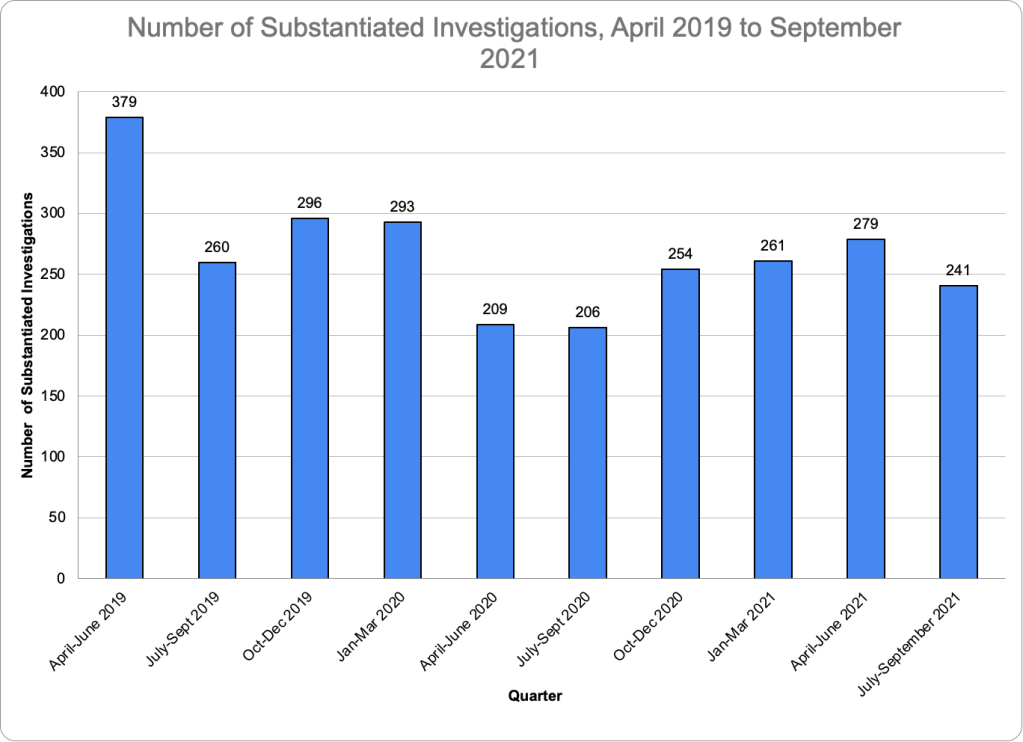
With fewer referrals accepted for investigation, there were naturally fewer investigations, as the height of the bars in Figure 4 shows.* The number of investigations that was substantiated (meaning the allegation of maltreatment was supported by the investigation) decreased from 861 in FY 2022 to 799 in FY2023, which was a drop of 7.2 percent. But the percentage of investigations that were substantiated did not change, remaining at about 21.5 percent of all investigations. So the decline in substantiations reflects the decline in the number of investigations initiated rather than a decreasing tendency to substantiate allegations.
Substantiated investigations can result in several outcomes, depending on the level of danger and risk to the child or children as estimated by Child Protective Services (CPS). if the child or children are deemed to be at low-or moderate risk, policy dictates that the family be referred to one of the Healthy Families/Thriving Communities collaboratives, nonprofits that are funded by CFSA to provide case management and other services. If the risk is deemed to be high or “intensive,” CFSA opens an in-home case. And if the child or children are assessed to be in imminent danger, the child is placed in foster care or an informal placement with kin or a family friend.**
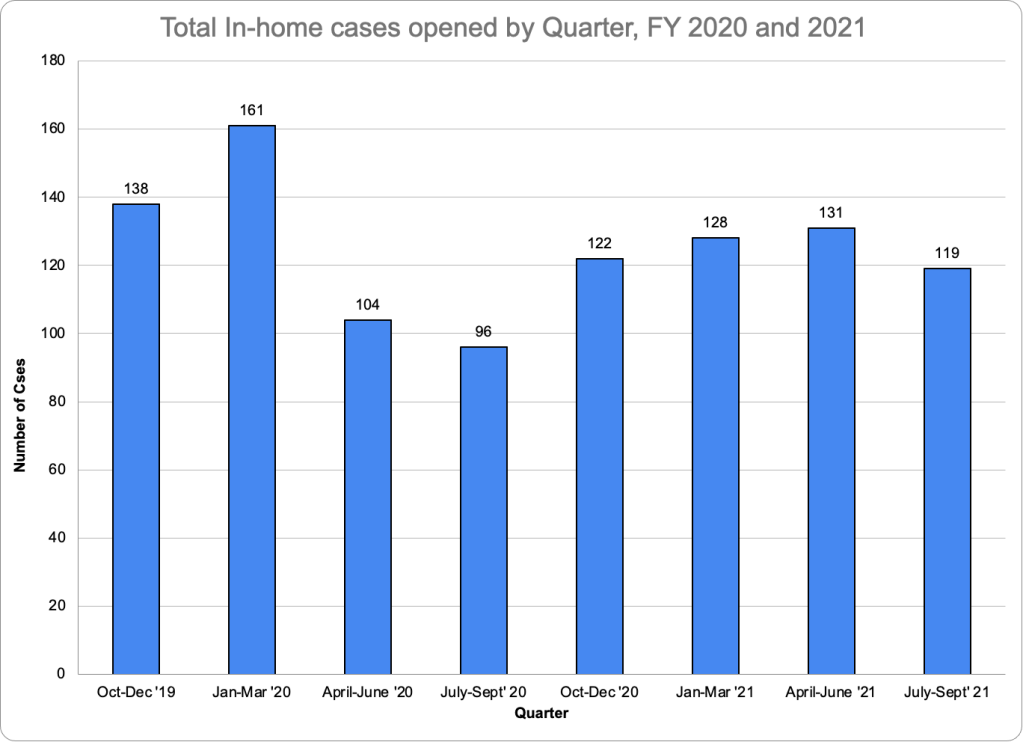
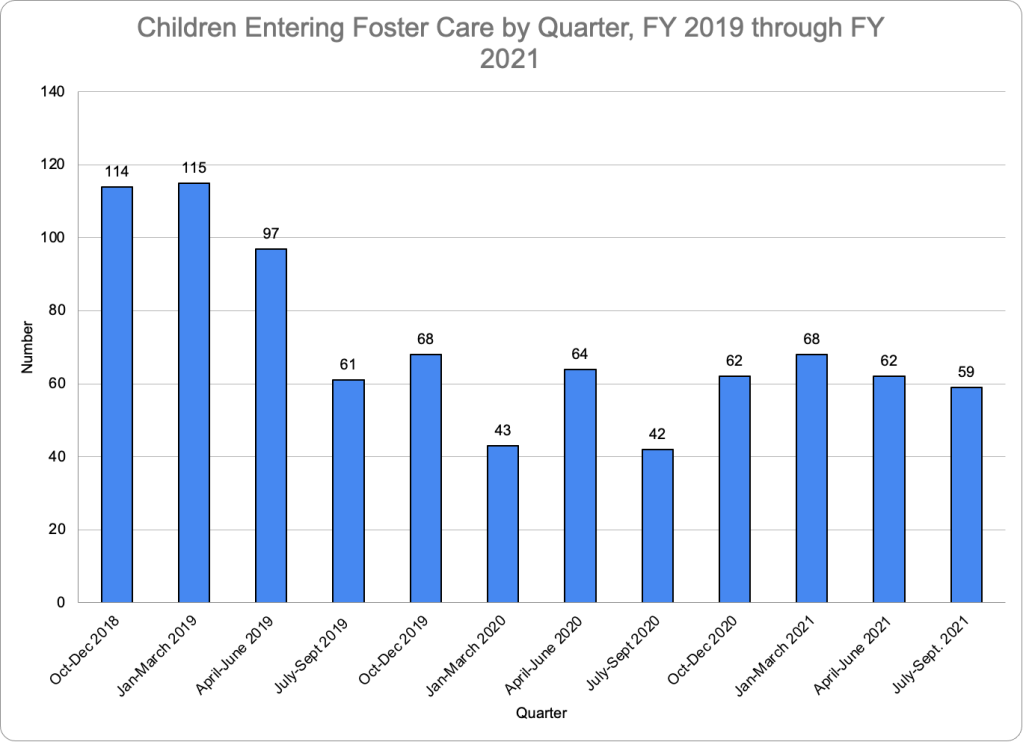
Table 1 shows the number of substantiated investigations, in-home cases opened, and foster cases opened between FY 2019 and FY 2023. The table shows that the number of substantiated investigations has been falling since 2020. In-home case openings fell moderately from FY2020 to FY2022 and dramatically from 463 in FY2022 to 363 in FY2023, a drop of 21.6 percent. Foster care entries, which had fallen rapidly between FY2019 and FY2022, fell less dramatically in FY2023, perhaps beginning a leveling trend after years of rapid decline. The total of in-home cases opened plus foster care entries (in other words, the total number of cases opened) fell from 886 in FY2019 to 542 in FY2023, a drop of 38.8 percent. From FY2022 to FY2023, total cases opened dropped by 18.4 percent. The number of In-home and foster care cases opened as a percent of substantiated investigations over the five-year period has dropped considerably since 2019, from 88.2 percent in FY2019 to 67.8 percent in FY2023, indicating a reduced likelihood of opening a case when an allegation has been substantiated.
Table One: Substantiations, In-Home Cases Opened and Foster Care Entries, FY2019 - FY2023
Fiscal Year
2019
2020
2021
2022
2023
Substantiated investigations
1004
1035
920
861
799
In-Home Cases Opened
499
500
442
463
363
Foster Care Entries
387
217
251
201
179
Cases opened (In-Home Cases Opened Plus Foster Care Entries)
886
717
693
664
542
Cases opened as a percent of substantiated investigations
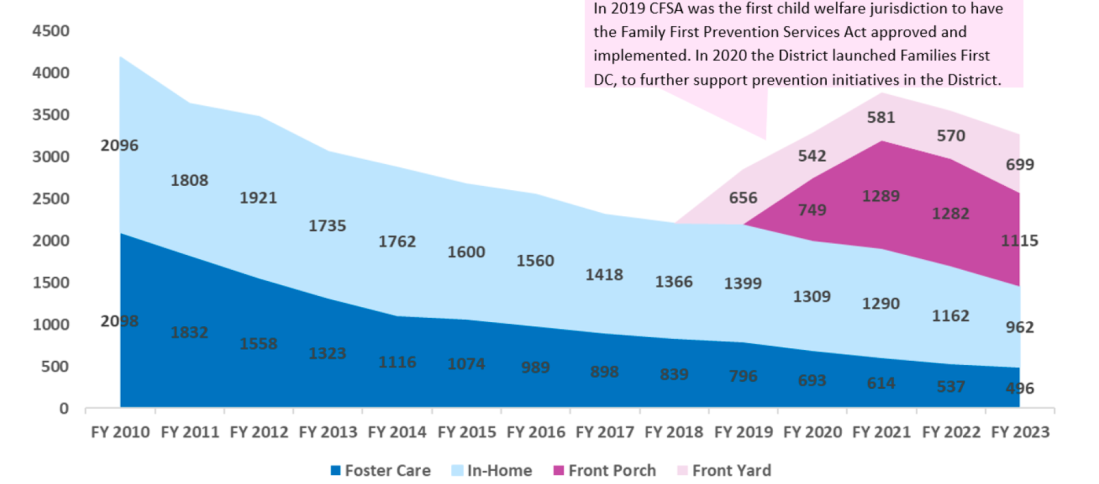
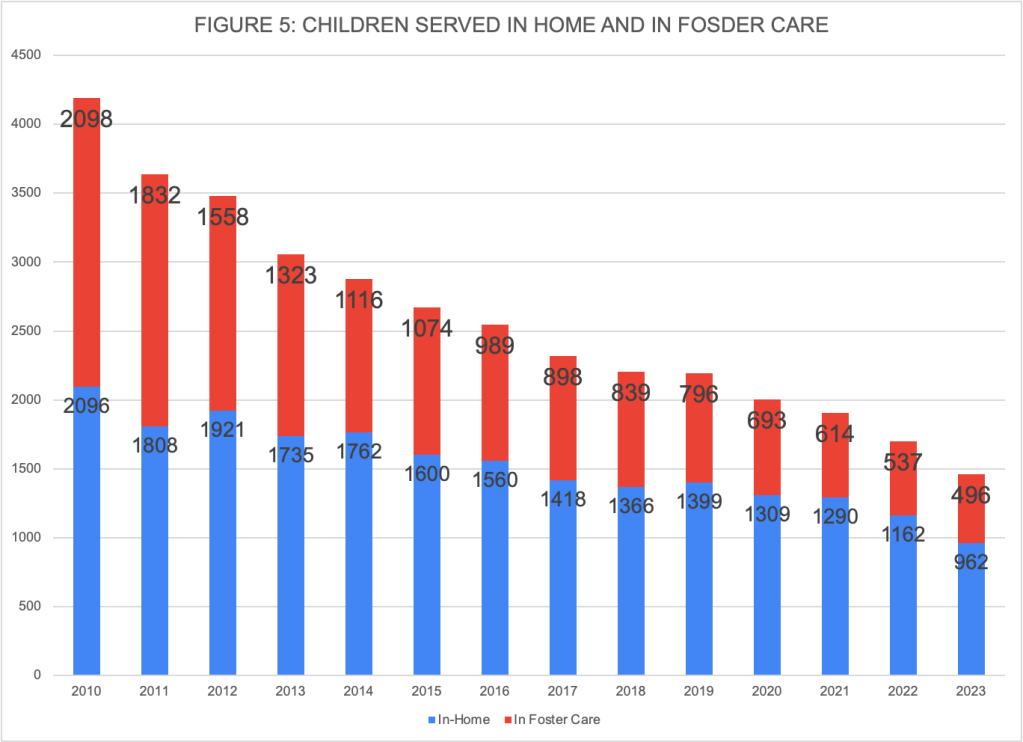
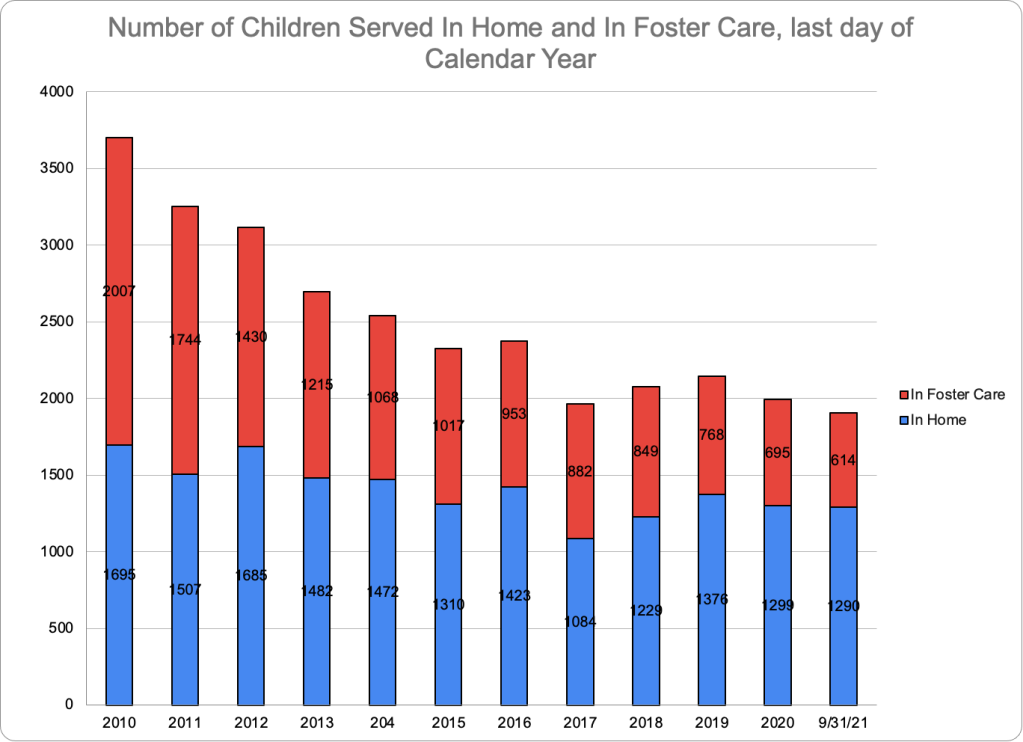
For a longer-term view, Figure 5 shows the number of children served in-home and in foster care on the last day of the fiscal year (September 30), using historical data from CFSA’s most recent Annual Needs Assessment.*** In 2010, about as many children were served in foster care as in their homes, but since that time the proportion of children served in their homes has risen, standing at 66.0 percent in September 2023. The foster care caseload has decreased every year and shows signs of starting to level off. The in-home population has also declined over time, though less steadily. The number of children served in their homes, though still much larger than the foster care population, has fallen much faster than the latter in recent years, dropping from 1,290 on September 30, 2021 to 962 on September 30, 2023. The total number of children served in home and in foster care has fallen from 4,194 in FY2010 to 1,458 in FY2023, a drop of 65 percent. And it dropped by a precipitous 33.6 percent between FY 2019 and FY2023. The “footprint” of CFSA, in terms of essential services, has shrunk dramatically.
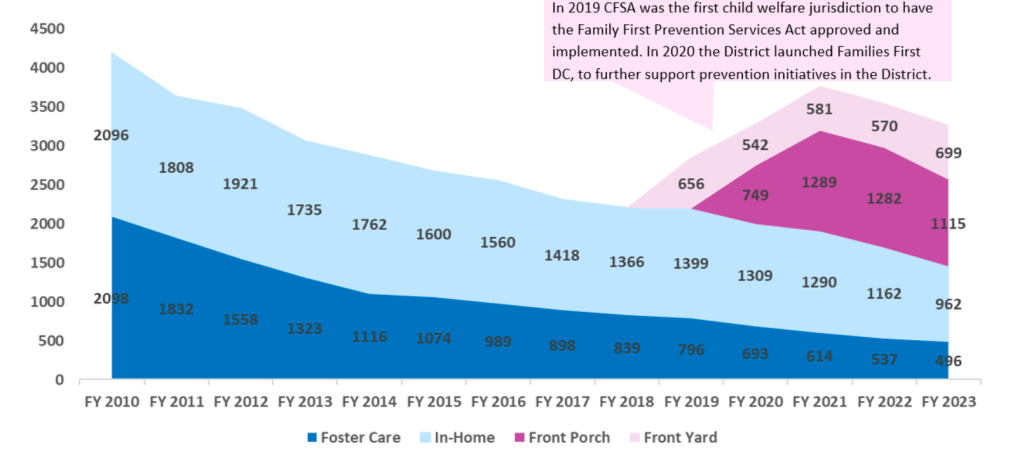
CFSA is pushing back against any impression that it is serving fewer families and children, as shown in the graphic displayed below from the latest Annual Needs Assessment. To the foster care and in-home populations (the same numbers shown in Figure 5) they add two more populations starting in FY 2019 — children and families they categorize as “Front Porch” and “Front Yard.” The agency defines “Front Yard” as families not yet involved with CFSA “but facing challenges that could put them at risk of coming to the agency’s attention.” It defines “Front Porch” as “families known to CFSA, both with and without an open case.”**** These “Front Yard” and “Front Porch Families” are being served by the Healthy Families/Thriving Communities Collaboratives using CFSA funds, rather than directly by CFSA.
Adding the “Front Porch” and “Front Yard” children to the children served in their homes and in foster care gives the impression that the number of children and families served has not fallen but in fact has increased in recent years. That may be technically true, but there are serious problems with that assertion. First, the total number of children served by the Collaboratives began declining in FY2021, and it is not clear what the future holds. Second, the services provided by the Collaboratives are typically much less intensive (and therefore cheaper) than CFSA’s in-home services. Collaborative case managers are generally not licensed Masters-level social workers and have much higher caseloads than CFSA in-home workers. Therefore, they often do not have the time or the skills to to provide the same level of services. Collaborative services have had a dubious reputation over the years; one of the first things I heard as a social worker at a private District agency managing CFSA foster care cases is how one could not expect any meaningful services from a collaborative. As a matter of fact, CFSA tried to end its contracts with the Collaboratives in FY2018 under the previous director, Brenda Donald. But the outcry from Collaborative staff and community members (perhaps recruited by the Collaboratives themselves) led her to renew the non-competitive contract for the collaboratives.
Third, it is not obviously sensible to divert CFSA funds to families in the “Front Porch,” and especially the “Front Yard,” when the agency is clearly not doing enough for the families currently receiving in-home services. The latest needs assessment focuses on in-home services and is sobering reading. In-home caseworkers responding to a survey reported that the most common barriers that caregivers display (daily parenting behavior, substance abuse, and mental health) barely change between the opening and closing of an in-home case. Only a quarter of the in-home cases reviewed by CFSA’s internal reviewers demonstrated “good progress.” CFSA concluded that the lack of progress in the other three-quarters of cases was due to the lack of parental engagement in services. CFSA’s responses to oversight questions from the Committee on Facilities and Family Services show that of the 503 in-home cases closed in FY 2023 and the first quarter of FY 2024, 214 (or 40 percent) of the families have already been the subject of a hotline call after the case was closed. My study of deaths of children known to CFSA between 2019 and 2021 showed that four of the deaths occurred while an in-home case was open for the family. Three other families had had one or more in-home cases that closed before the children died.
The data analyzed here show that from FY2010 to FY2023, CFSA has been serving fewer families with in-home services and foster care. In the last year, the decline continued even as calls to the hotline increased. During that last year, it is the rejection of a higher number of referrals and the reduced likelihood of opening a case when a referral is substantiated that account for the decrease in families served. But what is the actual cause of these trends?
There is more than one possible explanation for the rejection of more referrals and the opening of fewer cases for each substantiated referral. Like other child welfare agencies, CFSA is struggling with a staffing shortage. Perhaps the lack of staff in all units is constraining the ability to conduct investigations and staff the number of cases that are needed. That could result in hotline workers accepting fewer referrals and CPS workers referring more families to the collaboratives instead of to in-home services.
Another factor that is clearly at play is a changing perception of the agency’s purpose. CFSA’s leadership seems unenthusiastic about its primary mission of responding to child abuse and neglect. Agency management craves a less reactive role, adding the prevention of child maltreatment to the agency’s other responsibilities. As Director Robert Matthews likes to say, and repeated in his oversight testimony, he wants to transform CFSA “from a child welfare agency to a child and family well-being system.” That’s why the agency has gone even further beyond its core mission in its Families First DC initiative, attempting to reach even beyond the front yard to work with any family living in one of the disadvantaged communities where they have funded Family Success Centers that provide a wide variety of services and activities. But the agency seems to disregard the fact that these programs are likely to attract the families that are the least at risk of child maltreatment.
CFSA’s approach is in tune with the messages that are coming from the federal government and the powerful foundations and nonprofits that heavily influence the national child welfare agenda. These organizations disparage the “family policing” functions of child welfare and recommend, if not abolition, a drastic reduction in its traditional functions of investigations, in-home services, and foster care. By being in tune with the Zeitgeist, CFSA puts itself in the pipeline for grants, awards, and positive attention from the federal government and private funders. Moreover, CFSA leaders also appear believe passionately in the currently dominant orientation.
The allergy to “reactive” services is telling. Many agencies have reactive missions-police, firefighters, emergency rooms-and one could argue these are the most important services of all because they save lives and prevent serious injuries. The analogy with the police cannot be ignored. Police react to allegations of crime just as child welfare agencies react to allegations of child abuse and neglect. To prevent crime, we must not rely on the police, who are overburdened already and not trained and equipped to provide the services needed. Instead we must turn to a whole host of agencies dealing with education, public health, mental health, housing, income security and more-the same agencies that we must mobilize if we want to prevent child abuse and neglect.
It is still interesting to speculate on how the rejection of more hotline reports by hotline workers and the reduced number of referrals to in-home services by CPS workers has been (and is being) accomplished in practice. Both the acceptance of referrals and the assignment of a risk level are governed by actuarial assessment instruments. But as a former social worker in the system, I know that these instruments can be completed so as to obtain the desired response. Perhaps that is the answer or perhaps the instruments have been changed. I wish the Council’s oversight committee for CFSA would ask the agency this question.
CFSA’s data for FY2023 provide new evidence that the agency is withdrawing from its primary mission of protecting children who have already been abused or neglected in favor of reaching out to families that have not been reported to the agency. This is particularly evident from the decrease in referrals accepted for investigation, the decreasing proportion of open cases as a percentage of substantiations, and the increased emphasis on serving, through the collaboratives and the family success centers, families that are not currently involved with CFSA. With total budgetary resources decreasing, there is reason to fear that abused and neglected children are less protected every year as CFSA spreads its resources more and more thinly.
Notes
*While the number of referrals accepted for investigation was 3,902 in FY2023 according to the Dashboard’s Hotline Calls by Referral Type graphic, the total number of investigations displayed in the Investigations by Disposition graphic was 3,704. The reason for the difference is unclear. According to the Dashboard, “accepted for investigation” means that “the hotline call resulted in a new investigation being opened on the family.” So the two numbers should be the same.
**Such an informal placement may occur before substantiation as well.
***These data do not exactly agree with numbers that I have collected from the CFSA dashboard over the years. I have also noticed that Dashboard data for the same period, particularly in-home case data, has changed over time.
**** It appears that those with an open CFSA case qualify as Front Porch families if they are receiving collaborative services as well as in-home services from CFSA, but this is confusing and suggests the agency may be double-counting families by counting them in both the “in-home” and “front porch” populations. The agency cites a different definition of Front Porch families in its 2023 Annual Public Report, saying that the term refers to “families that have already been the subject of a CPS investigation but did not present with safety or risk levels that warranted opening a child welfare case.
Good afternoon! Thank you for the opportunity to testify today. My name is Marie Cohen and I live in Ward 6. After my first career as a policy analyst and researcher, I became a social worker and served in the District’s child welfare system until 2015. Soon after leaving that job, I joined the Citizen Review Panel on CFSA, on which I served for four years, and then the Child Fatality Review Committee, on which I served for six years. I began writing a blog, which later became Child Welfare Monitor. I am proud to say that my blog is read by some of the leading policymakers, advocates, and academics in the field. I take a child-centered approach, placing the safety and wellbeing of the child above all other considerations.
On October 22, 2022, police were called to Stanton Road, SE, for a report of an unconscious child. By the time they arrived, Journey McCoy had already been transported to United Medical Center, where she was pronounced dead.[i] According to WUSA-9, Sasha McCoy, the child’s mother, reported that around 8:30 a.m. her daughter came from the back bedroom of the house and said she was hungry. McCoy gave her a Jell-O cup and went back to sleep. Around 1 p.m. she was awakened to two of her four children rummaging in the refrigerator. Instead of feeding them she put both children down for a nap and went back to sleep on the couch. Such reports of parents sleeping through their children’s days, without regular bedtimes or mealtimes, are classic symptoms of what child welfare experts call chronic neglect. Sometime later, Ms. McCoy woke up again and found her child unconscious with yellow mucus coming out of her mouth.
On October 22, 2022, police were called to Stanton Road, SE, for a report of an unconscious child. By the time they arrived, Journey McCoy had already been transported to United Medical Center, where she was pronounced dead. According to WUSA-9, Sasha McCoy, the child’s mother, reported that around 8:30 a.m. her daughter came from the back bedroom of the house and said she was hungry. McCoy gave her a Jell-O cup and went back to sleep. Around 1 p.m. she was awakened to two of her four children rummaging in the refrigerator. Instead of feeding them she put both children down for a nap and went back to sleep on the couch. Such reports of parents sleeping through their children’s days, without regular bedtimes or mealtimes, are classic symptoms of what child welfare experts call chronic neglect. Sometime later, Ms. McCoy woke up again and found her child unconscious with yellow mucus coming out of her mouth.
During the ensuing investigation, police learned that Sasha McCoy, was known in her neighborhood for using drugs and being constantly high. McCoy admitted to using Percocet daily, including the morning of the day her daughter died. When the CFSA investigator offered her a referral to drug treatment she responded, “this is not the time. I am going to get high as a “mother f-er when I leave.” Seven months later, the autopsy came back. The cause of death was fentanyl intoxication. McCoy was arrested and charged with first degree felony murder and cruelty to children. During the fatality investigation, CFSA and police learned that the mother was living with a known drug dealer. She admitted to the use of unprescribed drugs, which she failed to secure away from the children. The dead child’s sibling has been placed in foster care.
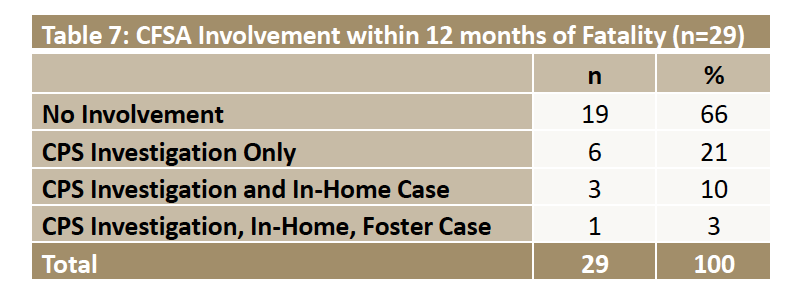
CFSA knew about McCoy before her daughter’s death, as described in the agency’s newest annual fatality report, which focuses on deaths of children in families known to CFSA in the previous five years.[i] Within five years of the three-year-old’s death, the family had three CPS investigations, one family assessment, and two open in-home cases. According to WUSA9, one of these cases was opened in 2020 when the same little girl as a baby ingested marijuana at a party McCoy was hosting. Social workers found three children unsupervised inside the home. The case was eventually closed. Another case was opened In August 2021 after McCoy’s newborn had symptoms of withdrawal. McCoy acknowledged using Percocet daily throughout her pregnancy. That case remained open until February 3, 2022, eight months before the fatality. Surprisingly, the agency did not observe any evidence of drug use or concerns for supervision during the two open in-home cases. (This is hard for me to believe, unless the mother evaded social worker visits, as happened with many of the cases I reviewed.) Nevertheless, CFSA reported that “case notes indicated the mother resisted the Agency’s efforts to engage her and she was inconsistent with participation in services.”
“We are not here to save children.” That is what I was told on the first day of my training as a child protective services worker at CFSA. And indeed, the District of Columbia is on the cutting edge of the current movement in child welfare that considers child protective services as a “family policing system” that unnecessarily harasses and separates families, especially families of color. But some families do not provide a safe environment for children to grow and develop. In some of these families, children die. That is what happened to the 16 children whose cases are discussed in my recently released report.
Why do I study fatalities among children known to CFSA? For the same reason that CFSA studies these deaths. As the agency states in its 2023 Annual Child Fatality Report, seeing where the system may have broken down helps it identify strategies that may prevent such deaths in the future, which is why the agency makes recommendations at the end of these reports. But it is more than that. The same conditions that lead to child fatalities also lead to harm for many more children. In that sense, child fatalities are the tip of the iceberg of child maltreatment, giving us a window on what is happening to other children who may be invisible to us.
The report is based on information I received from CFSA on the deaths of 16 children between 2019 and 2021—before the death I described earlier. These children came from families that had previous contact with CFSA. Their deaths were either ruled to be caused by child abuse or neglect or the Medical Examiner could not rule out child abuse or neglect as contributing to the cause of death.” District law requires the release of information on these deaths, but CFSA interpreted that law restrictively. Several deaths were not included because they were ruled to be accidents, although parental neglect clearly contributed to these deaths. For example, the death of seven-week-old Kyon Jones, whose mother told police that she threw his body in a dumpster after she rolled over him while high on PCP, was not included because his body was never found and could not be autopsied. A child was left in a baby swing for two hours was also included because his death was deemed accidental.
In addition to omitting some cases in which neglect or abuse played a role, CFSA heavily redacted the information it did provide, with many pages and large blocks of text blacked out. This included most information about the parents’ issues with drugs, alcohol, or mental health and almost the entire history of agency involvement in most cases. Despite the limited information provided, the redacted summaries included some disturbing new information.
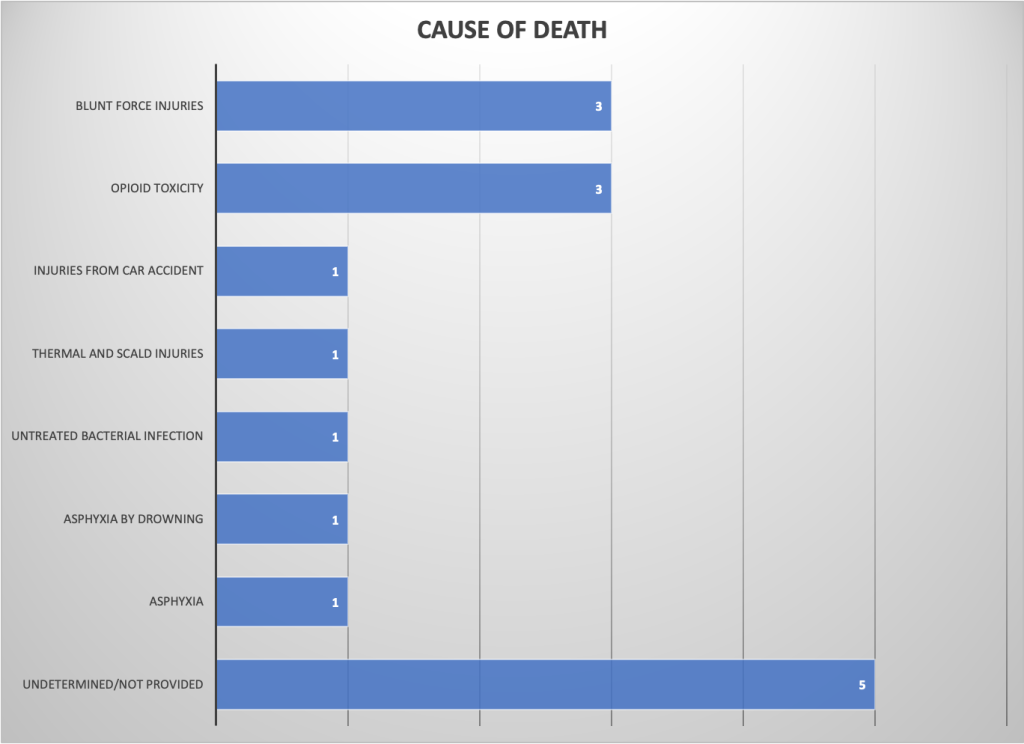
Causes of Death
The most common causes of death among the 16 children were blunt-force trauma and opioid poisoning, each claiming the lives of three children. This included Makenzie Anderson, who was murdered by her mother, and Gabriel Eason, who was the victim of long-term torture and beatings by his stepfather, as his mother stood by. The third case of blunt-force trauma was a three-year-old girl in the home of an aunt where she was placed by CFSA. Nobody has been charged for this murder. Another three children (a three-year-old girl, a three-year-old boy, and a three-month-old girl) died of poisoning by a controlled substance, with fentanyl implicated in all three cases. The remaining children died from drowning, asphyxia, “thermal and scald injuries,” injuries from a car accident, and unknown causes, a few of which may not reflect maltreatment.
Demographics
A quarter of the children who died were younger than six months old and half were one year old or younger. Another quarter were two or three. This is not surprising as young children are more vulnerable and similar results are found nationally. But older children were not invulnerable to abuse or neglect, including the seven-year-old who died in a car accident and a 12-year-old who died of an untreated bacterial infection and pneumonia.
All of the decedents were Black: fifteen were African American and one was classified as “African-biracial.” According to the latest data from Kids Count, 54 percent of children in the District of Columbia are Black. So Black children were overrepresented among the children who died of maltreatment or possible maltreatment. Yet, the District is trying to reduce racial disparities in system involvement. It sounds to me like a way to make Black children less safe, not more equal.
The prevalence of large families among those that lost a child due to abuse or neglect is striking, though not surprising, because research shows that large families are associated with child maltreatment. More than two thirds of the mothers of children who died by maltreatment had four or more children. The average mother in the group had 4.6 children, often with more than one father. This is not surprising, because larger number of children are associated with child maltreatment. The challenges of parenting multiple children clearly contribute to a child’s risk of being abused or neglected and dying of that maltreatment.
Histories of System Involvement
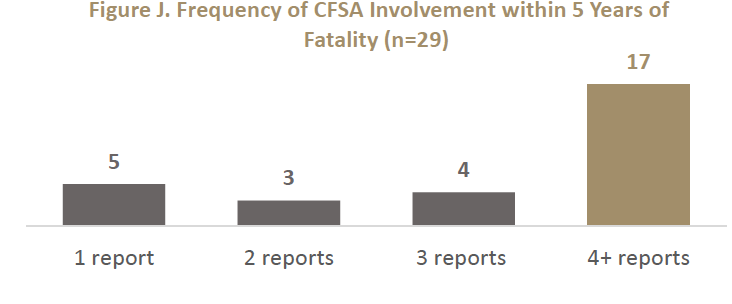
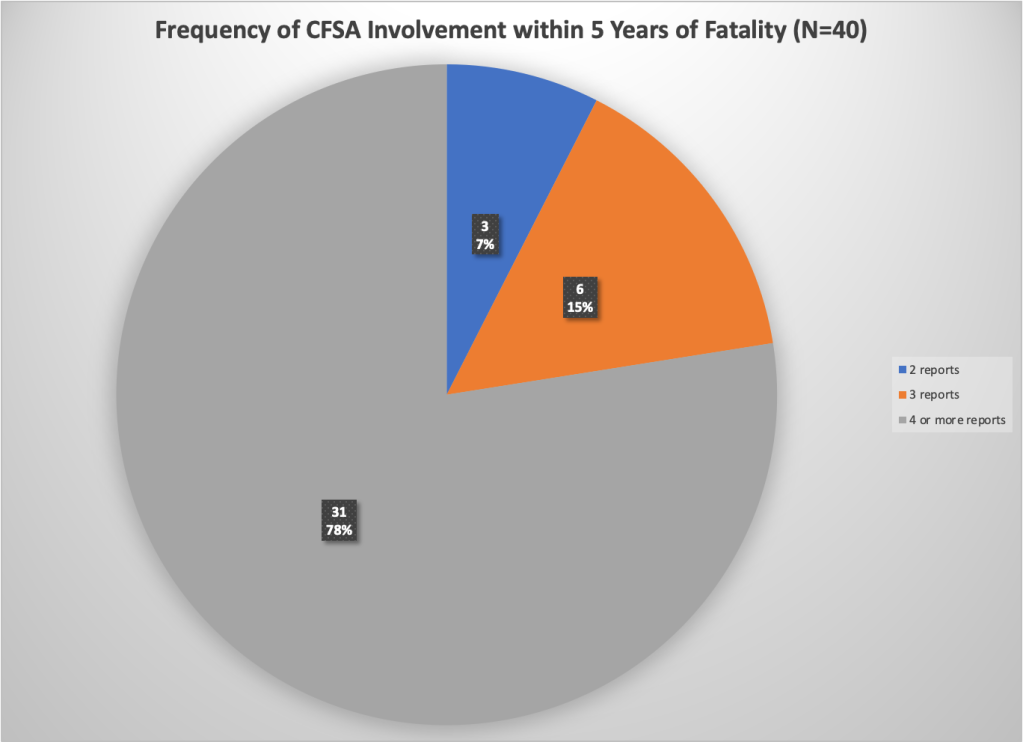
Most of the families that lost a child had experienced multiple reports prior to the fatality. Among the 16 fatalities included in this report, only six occurred in families that were the subject of five reports or fewer in the last five years. Five occurred in families that had between six and 10 reports, three occurred in families with 10 to 15 reports, and one family had 24 reports. Three of the families had experienced a previous child fatality–a shocking statistic considering the rarity of child fatalities overall.
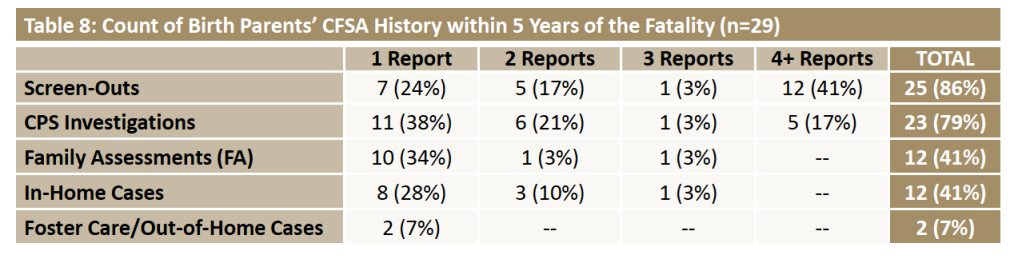
Substance abuse by the parent or caregiver (including positive toxicology of a newborn) was the most frequent allegation CFSA received regarding the families in the five years before the deaths. Substance abuse by the parents was observed or alleged in the families of all but four of the victims included in this report. Inadequate supervision and educational neglect were the next most common. Ten of the 15 families had at least one report for educational neglect and ten for inadequate supervision before the child’s death. Another major theme was exposure to domestic violence, which was mentioned in nine of the 16 case histories as the subject of an allegation or in notes from social workers or police.
A 17-month-old boy died of “thermal and scald injuries.” His mother had no idea how he got injured. She said he was sleeping on the floor next to her bed when she went to sleep at 7:00 PM, but he often slept next to the radiator in the living room because she kept the air conditioning on high and he got cold. She reported that one of her five other children woke her at about 3:00 AM and showed her large pus bubbles on the child’s thigh and lower leg. She told the girl to bring him to another room and planned to clean the wound in the morning, for fear of being reported to CFSA. She reported having no idea why he was found in the bathtub with his face down at about 7:00 AM.
System Failures
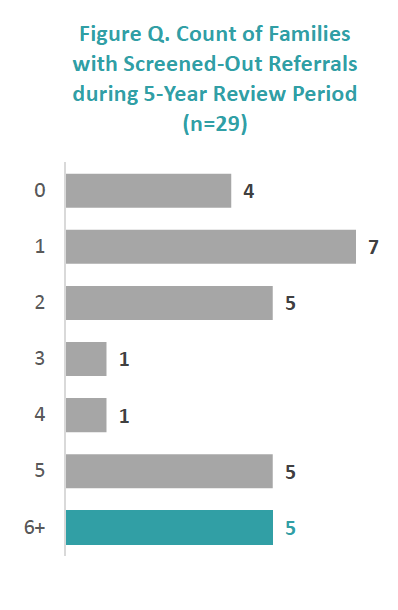
The information received suggests several areas where failures in policy and practice by CFSA may have allowed these deaths to happen. These areas include screening and investigation. Many reports on these families were screened out hotline staff, perhaps inappropriately. The Office of the Ombudsperson for Children (OFC) reports that it received complaints from constituents about referrals that were screened out inappropriately; OFC itself had concerns about several referrals that were screened out. OFC also heard from school staff who reported receiving no feedback after submitting multiple reports on the same family.
Flawed investigations may have also allowed these fatalities to happen, as these families had many unsubstantiated investigations. The details of most investigations were completely redacted, so I cannot give many examples of possible flaws. But Gabriel Eason, who was beaten to death by his stepfather, was the subject of an investigation five months before his death, after he showed up at childcare with two bruised ears. The CPS investigator did not seem concerned about the mother’s lack of knowledge of how the injury was acquired, her offering of multiple possible explanations, and the question of how playing rough with his siblings on running into furniture could result in bruises on both sides of his face.
Management of in-home cases was revealed by these fatalities as an area of concern for CFSA. Four of the deaths I reviewed here happened while an in-home case was open for the family, yet in three of these cases, workers struggled to complete face-to-face visits with the families because parents evaded these visits. Three other families had had one or more in-home cases that closed before the children were killed. In the Needs Assessment it recently released, CFSA focused on its in-home services and found little evidence for optimism about their potential to help children. By caseworkers’ own assessment, the most common barriers that caregivers display (daily parenting behavior, substance abuse, and mental health) barely change between the opening and closing of an-In-Home case. Only a quarter of the In-Home cases reviewed by CFSA’s internal reviewers, demonstrated good progress according to these reviewers, despite the good clinical skills of the social workers. CFSA concluded that the lack of progress in the other three-quarters of cases was due to the lack of parental engagement in services.1 CFSA’s oversight responses show that of the 503 in-home cases closed in FY 2023 and the first quarter of FY 2024, 214 (or 40%) of the families were the subject of a hotline call after the case was closed.
In the three open cases where parents evaded social worker visits, social workers and supervisors could have used the “community papering” option to file a petition to involve the court. But they did not exercise this option–or they started too late. In one case, a three-year-old had been left alone on her stomach with a bottle while her mother went across the street to retrieve and smoke a cigarette. During the in-home case resulting from that fatality, the case manager made multiple unsuccessful attempts to see the mother and her three surviving children. Due to the mother’s failure to engage and the children’s continued absence from school, the case manager scheduled a meeting with legal staff to consider community papering. That meeting was scheduled for December 8, 2021 and was canceled after CFSA learned of the three-year-old’s death of fentanyl poisoning on December 3.
In the FY2025 Needs Assessment, CFSA stated that “[h]istorically, QSR reviews have shown that parents’ active participation and engagement in services, and their ambivalence to work with the Agency, remain a challenge for the In-Home Administration. Despite training inevidence-based skills [such as motivational interviewing] social workers continued to face multiple challenges for achieving positive outcomes. . . Challenges for the social work team and the families included complicating factors such as unresolved (or insufficiently addressed) family histories of trauma, substance use, mental illness, cognitive challenges, and parenting capacity with multiple children.
Recommendations
The Council should change the law to mandate release of Information on child maltreatment fatalities. Sadly, CFSA’s internal fatality committee, which reviewed the full record of these cases, does not do a good job of making recommendations. The 2022 report had no recommendations for CFSA other than it should participate in districtwide discussions about violence prevention; its other recommendations referred to other agencies, like better information sharing and a safe sleep campaign. We certainly cannot rely on CFSA to learn from its mistakes. Therefore, my first recommendation is to the City Council, urging it to require that CFSA follow the example of states like Florida, Arizona, and Wisconsin, andrelease detailed historical information on child fatalities, with certain identifying information redacted.
CFSA should Improve the hotline and investigations through training and specialization: I endorse the OFC’s recommendation for enhanced training for hotline staff so that reports are screened adequately to ensure the safety of children. In addition, school absences should be investigated regardless of the age of the child (requiring a change in the law) and their academic performance. Investigative workers could benefit from better training in forensic interviewing techniques that might help them better evaluate parents’ and children’s’ statements for veracity and perceive more subtle signs of abuse or neglect. Another option is to reinstate the Special Abuse Unit so that cases of physical and sexual abuse are handled by workers with forensic interview training.
CFSA must recognize that in-home cases need to be more intensive and longer for chronically neglectful families: CFSA must also strengthen its in-home practice, perhaps by reinstating the Chronic Neglect Units, which were eliminated barely a year after they were implemented. These units would employ specially trained social workers with lower caseloads and longer time periods to work with families.
The agency must reduce any barriers to the use of “community papering,” perhaps making court involvement routine after a certain number of missed visits or other instances of noncooperation, or if a family that is offered in-home services after an investigation refuses the offer. The case narratives make clear that social workers struggled to complete home visits to the families of the children who later died, and yet community papering was either not initiated, or initiated too late. According to the recent Needs Assessment, the agency presented over 300 children with in-home cases for community papering in FY 2021, FY2022 and the first quarter of FY2023.[iii] But my study suggests that these petitions must be made sooner and more often.
It is often said that we should not make policy based on extreme cases. But I have a different view. Extreme cases are the tip of the iceberg. Every child who dies, represents multiple other children who are suffering or at least failing to thrive as they live with abuse or neglect. Studying fatalities can help identify system failures that allow many more children to languish in abusive or neglectful homes, growing up in fear or pain, or without the essential nurturing necessary for normal child development.
CFSA also found that when an In-Home case is opened, a family’s risk of child removal decreases by 15 percent within a year. But the likelihood of a new investigation increases by 10 percent within the year. CFSA speculates that perhaps the subsequent Investigation ends up prolonging the in-home case by starting a new In-Home episode.
“We are not here to save children.” That is what I was told on the first day of my training as a child protective services worker at the District of Columbia’s Child and Family Services Agency (CFSA). And indeed, the District is on the cutting edge of the current movement in child welfare around the country that considers child protective services as a “family policing system” that unnecessarily harasses and separates families, especially families of color. The problem with this perspective is that some families do not provide a safe environment for children to grow and develop. In some of these families, children die. That is what happened to the 16 children whose cases are discussed in a new report, which is summarized in this post. And indeed, analysis of the limited information provided suggests that CFSA did not take advantage of the opportunities it had to protect children even after long histories of CFSA involvement in their families. As a result, three children were beaten to death, three more were poisoned by opioids, and others died of burns, a car accident, and unknown causes when the deaths might have been preventable if the agency had been more protective.
When a child dies of abuse or neglect after that child’s family has been on the radar of the agency designed to protect children, it is important for the public to know whether and how this death could have been avoided. The essential question is whether the agency could have prevented the death by doing something differently. Did staff miss any red flags, and therefore fail to take action when necessary? If the death was preventable, what factors must be remedied in order to prevent such failures in the future? It is not enough for the agency itself to have access to this information, or to have an internal team review it. Agencies can fail to learn from their mistakes when they are blinded by ideology, self-interest or just inertia.
For those reasons, federal law requires every state to have a law or program that includes “provisions which allow for public disclosure of the findings or information about the case of child abuse or neglect which has resulted in a child fatality or near fatality.” In compliance with this requirement, DC Code requires the Mayor or the Director of CFSA, upon written request or on their own initiative, to provide findings and information related to “[t]he death of a child where the Chief Medical Examiner cannot rule out child abuse, neglect, or maltreatment as contributing to the cause of death.” In March 2023, we requested such findings and information for all the fatalities that met the criteria and were reviewed by CFSA’s internal fatality review team between 2019 and 2021. It took more than six months of meetings and emails to receive the information that is presented in this report. We agreed to restrict our request to cases reviewed in 2019, 2020 and 2021 and to withdraw our request for information on near-fatalities, which CFSA only began tracking in October, 2022.
Not surprisingly, CFSA interpreted the disclosure requirements in a way that restricted the information provided as much as possible. If a medical examiner did not rule the manner of death to be an abuse or neglect homicide or “undetermined,” no information was provided. Therefore, the agency did not release any information on cases where the manner of death was labeled as accidental, even if it found a parent responsible for the death or removed the children. The “accidental” deaths for which information was not provided included one child who died after he was left in a baby swing for two hours, which most ordinary people would consider to be neglect. The death of seven-week-old Kyon Jones, whose mother told police that she threw his body in a dumpster after she rolled over him while high on PCP, was not included because his body was never found and therefore it did not meet the criteria for release of the information–even though CFSA removed the surviving children from their mother.*
In addition to omitting some cases in which neglect or abuse played a role, CFSA heavily redacted the information it did provide, with many pages and large portions of others blacked out. CFSA refused to provide the names of the children, parents and caregivers, providing a rather convoluted interpretation of DC Code, which clearly requires the release of this information. (See the full report for more information about their reasoning). In three cases, the child’s identity was clear from media coverage of the case, and we used the child’s name. A major source of redactions was the exclusion of “personal or private information unrelated to the child fatality.” It appears that CFSA’s legal team interpreted this term much more broadly than a social worker or researcher would, because they redacted almost all information about parents’ history of criminal activity, substance abuse, mental illness, and domestic violence–which are obviously relevant to many of the fatalities we are discussing.
On investigations, it is unfortunate that DC Code requires that the agency release only ”a description of the conduct of the most recent investigation or assessment” rather than all investigations regarding the family in question. It appears that the agency interpreted “the most recent investigation” as the fatality investigation itself rather than the most recent investigation before the fatality, but the law ought to require a description of all previous investigations. The agency also disregarded language that requires it to provide “the basis for any finding of either abuse or neglect.”
For most cases, we received very little information aside from a list of the previous referrals (reports to the CPS hotline) including only the date of the report, the allegation category and the disposition; an account of in-home and foster care case activities for the families that had such cases; and an account of the investigation of the fatality itself. The information about the parents was heavily redacted, and almost the entire history of agency involvement was blacked out in most cases. Despite the limited information provided, the redacted summaries included some new information, some of which was startling and disturbing. The report is based on the 16 case summaries provided by CFSA, occasionally supplemented with information from the agency’s annual fatality reports, which are available to the public. These cases affected 15 families, as one family had two fatalities in one year. Unless otherwise noted, the information is based on the case summaries. The full report, from which this blog is excerpted, contains summaries of each case.
Cause and Manner of Death
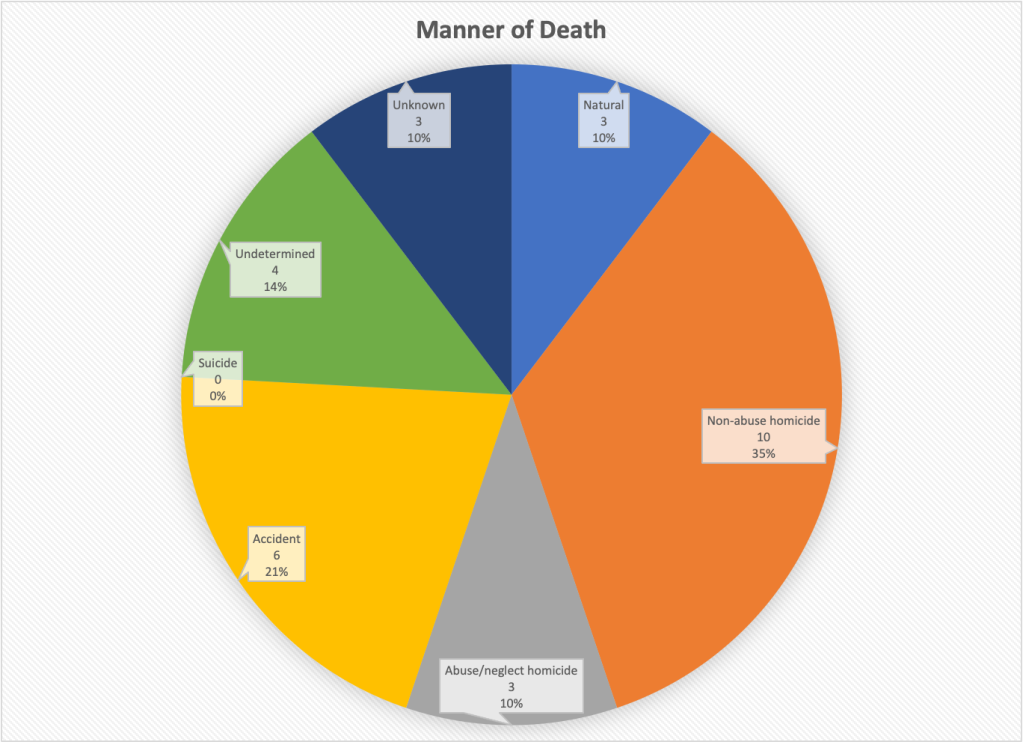
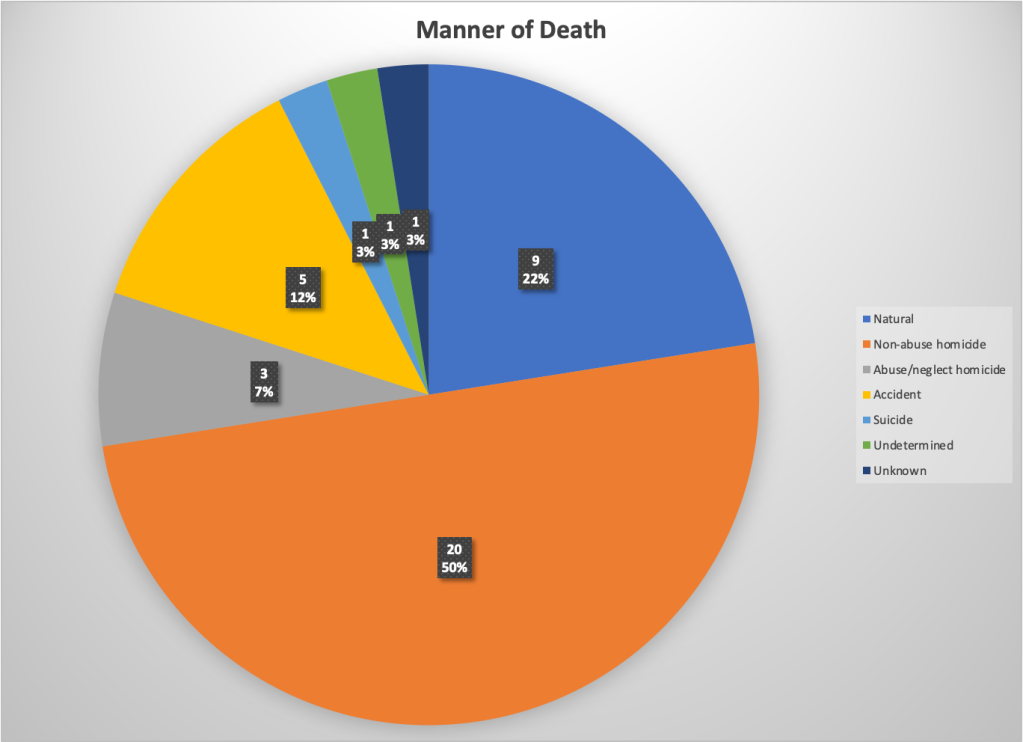
CFSA classifies child deaths by cause and manner. “Cause of death” is the specific disease or injury that led to the death. Manner of death refers to the circumstances that caused the death, and falls into five categories: natural, accidental, suicide, homicide, and undetermined. Of the 16 cases for which information was provided by CFSA, three (19 percent) were abuse homicides, six (37 percent) were neglect homicides, and seven (44 percent) were undetermined in manner. The latter were the cases for which CFSA provided information because the Medical Examiner was unable to rule out child abuse or neglect homicide as the manner of death.
The most common causes of death were blunt-force trauma and opioid poisoning, each claiming the lives of three children, as shown in figure below. The remaining children died from a variety of causes, including drowning, asphyxia, thermal and scald injuries, injuries from a car accident, and unknown causes.
Abuse deaths: Blunt Force Trauma
Three of the children died of blunt force trauma-one of the two most common causes of death in the sample. The murders of two of these children - Makenzie Anderson and Gabriel Eason - - became known to the horrified public through press coverage of their deaths in February and April of 2020. Each of them died from head trauma inflicted by a parent or stepparent. Makenzie suffered from multiple contusions to the face and head, skull fractures, and other injuries, and her mother pleaded guilty to manslaughter, receiving a ten-year prison term with seven years suspended on the condition that she obtain mental health treatment and have no unsupervised contact with children. Gabriel’s autopsy found abrasions and contusions to the head, face and torso; contusions to the heart and thymus gland; liver and kidney laceration; new and healing fractured ribs; and a brain hematoma. His stepfather was sentenced to 12 years and eight months in prison and his mother, who did not seek medical help for Gabriel or his critically-injured three-year-old brother, was sentenced to four years of probation and three years of supervised release.
But there was a third homicide by blunt force trauma. A three-year-old girl died of trauma to the abdomen in the home of an aunt where she was placed by CFSA after being removed from her drug-addicted mother. Her injuries included contusions to the forehead and abdomen, a lacerated liver, and blood in the abdominal cavity. No charges were filed against either the aunt or her boyfriend, and the case received almost no public attention.
Neglect deaths: Opioid Poisoning and other causes
Three children (a three-year-old girl, a three-year-old boy, and a three-month-old girl) died of synthetic opioid toxicity, with fentanyl implicated in all three deaths. (One of the children had also ingested a controlled substance called eutylone.) There is no information about how the children might have ingested the drugs, but all lived with parents who were known or alleged to abuse substances. These deaths never became known to the public, which is not surprising since it appears that none of the parents were arrested or charged.
A 17-month-old boy died of “complications of thermal and scald injuries,” and his mother told the investigator that she had no idea how it happened or how he ended up face-down in the bathtub several hours later. A seven-year-old died of injuries from a car accident. His mother was a long-time substance abuser and was arrested for Driving Under the Influence (DUI) in the accident. She was driving from Florida to Washington and her children were not sitting in car seats or belted in. A five-month-old boy died of asphyxia by drowning after being left alone in the bathtub with a one-year-old sibling while their mother searched for her car keys.
Deaths for Which the Manner was Undetermined
Two deaths has known causes but the manner - whether abuse or neglect or something else - was not determined. A twelve-year-old girl with asthma died of an untreated bacterial infection and pneumonia but also had enough bruising from two separate beatings in the previous two days to support a CFSA substantiation of the mother for physical abuse. It is unclear why this was not considered a medical neglect homicide. A ten-month-old girl died of asphyxia but the manner of death was undetermined. Her mother had left her in the care of her father and returned to find her unresponsive.
The cause as well as the manner of death was unknown or undetermined in five cases. These included an 18-month-old boy with a subdural hematoma, which could have been caused by abuse or a fall, an 11-month-old girl whose mother reported leaving her unsupervised on her stomach with a bottle in her mouth for about 40 minutes, a nine-month-old boy put to bed with a bottle and found face-down on a pillow; a two-month-old girl who died while sleeping with her mother, and a three-month-old girl found unresponsive by her parents one morning. Unsafe sleep practices may have contributed to some of these deaths, but other unsafe sleep fatalities were categorized as accidents, for which case summaries were not provided.
Demographics
A quarter of the children who died were younger than six months old and half of them were one-year-old or younger. Another quarter were two or three. This is not surprising as young children are more vulnerable and similar results are found nationally. But older children were not invulnerable to abuse or neglect, including the seven-year-old who died in a car accident and the 12-year-old who died of an untreated bacterial infection and pneumonia.
Fifteen of the decedents were African American and one was classified as “African-biracial.” According to the latest data from Kids Count, 54 percent of children in the District of Columbia are Black. So Black children were overrepresented among the children who died of maltreatment or possible maltreatment. The overrepresentation of Black children among children who died points to Black children’s particular need for protection. And it suggests that current emphasis in the District and around the country on reducing the involvement of Black families in child welfare may cause more suffering and more deaths among Black children.
The prevalence of large families among those that lost a child due to abuse or neglect is striking. More than two thirds of the mothers of children who died by maltreatment had four or more children. The average mother in the group had 4.6 children, often with more than one father.
Histories of System Involvement
All the families had been the subject of at least one report to the CFSA hotline before the fatality, or else they would not be included in this report. But many of the families that lost a child had experienced a large number of reports prior to the fatality. Among the 16 fatalities included in this report, only six occurred in families that were the subject of five reports or fewer in the last five years. Five occurred in families that had between six and 10 reports, three occurred in families with 10 to 15 reports, and one family had 24 reports. Three of the families had actually experienced a previous child fatality–a shocking statistic considering the rarity of child fatalities overall.
The families of the two children - Makenzie Anderson and Gabriel Eason - whose abuse homicides shocked the District of Columbia in February and April 2020 were both known to CFSA before the deaths, and the last report to the hotline came five months before the fatalities of both children. Makenzie Anderson’s family was reported to the hotline eight times within five years of her death. The last report alleged exposure to unsafe living conditions, inadequate supervision, and substance abuse by a parent, caregiver, or guardian. All those allegations were unfounded (not confirmed) by CFSA. Gabriel Eason’s family was the subject of 17 prior calls to the hotline since 2012, including 12 in the five years preceding Gabriel’s death. The most recent report was for unexplained physical injury in October 2019 and was also unfounded by CFSA.
Substance abuse by the parent or caregiver was the most frequent allegation CFSA received regarding the families in the five years before the deaths, with 30 substance abuse allegations collectively accumulated by the families of the 16 dead children during that period. Another eight reports concerned positive toxicity of a newborn, a reflection of parental substance abuse. Substance abuse by the parents was observed or alleged in the families of all but four of the victims included in this report. Inadequate supervision was the second most common allegation, with 25 allegations concerning the 15 families. Almost as common was educational neglect, referring to children with excessive school absences, with 24 allegations received in the five years preceding the fatality. Ten of the 15 families had at least one report for educational neglect before the child’s death. Another major theme was exposure to domestic violence, with 17 allegations received by the families. Domestic violence was mentioned in nine of the 16 case histories as the subject of an allegation or in notes from social workers or police.
Most of these families could be described as “chronically neglectful.” According to the Child Welfare Information Gateway, “Chronic child neglect occurs when a caregiver repeatedly fails to meet a child’s basic physical, developmental, and/or emotional needs. Chronic neglect can have long-term, negative consequences for child health and well-being.” Working with chronically neglectful families is especially difficult and requires special training and skills, which many CFSA social workers may lack. Perhaps that is one reason why they struggled so hard to engage some of these families. Four of the children died while an in-home case was open. Three out of four of the in-home case narratives from CFSA portray caregivers who evaded offers of help from CFSA and other providers and refused to cooperate with efforts to monitor conditions in their homes.
System Failures
The information received suggests several areas where failures in policy and practice by CFSA and other agencies may have allowed these deaths to happen. These areas include:
Screened out and unsubstantiated reports: Research points to the difficulty of determining correctly whether a child has been maltreated, as well as the absence of significant differences in subsequent outcomes between children with a substantiated allegation of maltreatment and those with an unfounded allegation. Without information on how hotline and investigation decisions were made, we cannot assess the agency’s performance in these areas. But the fact that most previous reports for families with a subsequent death were screened out or unfounded is concerning.
Flawed management of in-home cases: Four of the deaths reviewed here happened while an in-home case was open for the family. In three of these cases, workers struggled to complete face-to-face visits with the families because parents evaded these visits. Social workers and supervisors could have filed a petition to involve the court, an option known as “community papering.” But they did not exercise this option–or they started too late, as in the case of the child who died after a meeting was finally scheduled to discuss community papering the case. The meeting was cancelled after the agency received word of the child’s death.
Too many chances: The mother of the seven-year-old killed in the 2020 car accident had been given numerous chances to recover from drug addiction and had relapsed many times over 18 years of involvement with CSFA. The family of the 17-month-old who died of complications of thermal and scald injuries had 24 referrals to CFSA between 2016 and 2021. Three in-home cases were opened and closed, but the children were not removed until the little boy died.
A fragmented health care system: In its findings on Gabriel Eason’s death, CFSA pointed out that Gabriel was taken to different medical providers for his various injuries. Because they use different information systems, the providers could not see records of the earlier injuries.
The reaction of CFSA and the criminal justice system after the fatalities obviously did not contribute to the fatalities themselves but may illustrate a pattern that contributes to future deaths. Specifically, CFSA’s tendency to place siblings informally after fatalities and the police and US District Attorney’s failure to charge parents raise concerns.
Informal placements after fatalities: CFSA, and child welfare agencies around the country, have been criticized for relying on informal placements with family members, rather than formally removing the children, placing them with the relatives, and opening a case to monitor their safety and well-being. In at least four of the 16 cases reviewed here, CFSA did not officially remove the siblings of the children who died but instead relied on informal placements with fathers or other relatives to keep them safe. Nothing was done to assure that the children were not returned to the home from which they had been removed as soon as the investigations closed, or to verify that the parents or caregivers had rectified the conditions leading to the child deaths.
Failures by the criminal justice system: The failure to bring charges against some of the parents and caregivers described here is quite concerning, particularly in the case of the three-year-old who died of blunt-force trauma and the infant and two three-year-olds who died of opioid poisoning. There has been considerable criticism of the US Attorney’s office in the District (which handles adult criminal prosecutions) for its low rate of opting to charge people for crimes. We do not know if the problem is the Metropolitan Police Department’s failure to bring the cases to the US Attorney or the latter’s failure to pursue them.
Recommendations
Without seeing the full case studies that were available to CFSA’s internal review committee, we cannot make detailed recommendations about how to avoid child maltreatment fatalities for children known to CFSA. The minimal recommendations that CFSA’s internal review team made show the need for the City Council, advocates and the public to have access to these complete case studies. Therefore, our first recommendation is to the City Council, urging it to require that CFSA release comprehensive case histories on all proven or suspected child maltreatment fatalities: in its 2021 report the agency made no recommendations other than those dealing with the fatality review process! . Our next blog post will discuss the legislative changes that are needed.
The lack of information on how screening and investigation decisions in particular were made precludes specific recommendations. Perhaps a new audit of the hotline is in order. Some changes to hotline screening policy might be advisable, especially around educational neglect. School absences should be investigated regardless of the age of the child (requiring a change in the law) and their academic performance. And perhaps investigative workers could benefit from better training in forensic interviewing techniques that might help them better evaluate parents’ and childrens’ statements for veracity and perceive more subtle signs of abuse or neglect.
The case narratives make clear that in-home social workers struggled to complete home visits to the families of the children who later died. The agency must change its policy to encourage “community papering,” making court involvement routine after a certain number of missed visits or other instances of noncooperation. CFSA might also want to consider strengthening its in-home practice, perhaps by reinstating the Chronic Neglect Units, which were eliminated barely a year after they were implemented. These units would employ specially-trained social workers with lower caseloads and longer time periods to work with families.
Despite the current ideology favoring family preservation and reunification at all costs, the agency must also recognize that sometimes it must give up on a parent and find a safe, permanent alternative for the children. Giving parents multiple chances with successive children over many years belies the true purpose of child welfare services – to protect children.
Not all needed changes fall in CFSA’s bailiwick. Reforms in the criminal justice system are also necessary to ensure that parents who killed one child cannot harm more children. Couples who refuse to cooperate with prosecutors, and parents who expose children to opioids due to their own abuse or drug dealing must also be charged. Other jurisdictions do it, and the District must do it as well.
DC Health and medical providers also have a crucial role to play in making children safer. Encouraging the adoption of a comprehensive medical information platform across the region to prevent families from using different doctors to hide abuse and neglect would be a welcome step. A campaign by DC Health to educate young women on how an early pregnancy, especially when followed quickly by others, compromises their future and that of their children, is a crucial necessity. It must be accompanied by improved access to long-acting reversible contraceptive methods.
In summary, even with the very minimal information we received, some conclusions emerge. CFSA’s extreme deference to parents and guardians emerges clearly through the redactions in these narratives. This is in direct contrast to the picture that is being painted by the foundations, advocacy groups and public agencies dominating the child welfare conversation. Their accounts portray interventionist child welfare agencies that remove children rather than giving their families the help they need and want. We are seeing the opposite here: families who evade offers of help from the agency and providers and refuse to cooperate with efforts to monitor conditions in the home. The goal of such parents often appears to be to avoid surveillance by outsiders rather than to improve their ability to care for their children. And CFSA workers often seem unwilling or unable to intervene in a way that will protect these children.
‘The tragic deaths of children whose families are known to CFSA are the tip of a much larger iceberg. For every child who dies of abuse or neglect, an unknown number of others are living in fear or pain from abuse, suffering chronic neglect that will cause lifelong intellectual an emotional damage, or lacking the loving attention necessary for optimal mental, emotional and physical development. Sadly, it is only the children who die whose cases can be used to learn lessons to prevent similar tragedies in the future. This information must be public, so that the public can push for a system that protects all children who are not receiving the parental care they need to survive and thrive.
*The case, which received media coverage, was included and easily identifiable in
In the public testimony on the CFSA budget, there were pleas from several speakers to increase funding for home visiting programs funded by CFSA. So I did a little digging to determine how the current funds are being spent, and what I found was rather shocking. In Fiscal Year 2022 (FY22), CFSA handed over $330,000 to the DC Department of Health, to serve a grand total of 33 families, of whom only 16 completed the program. The agency spent another $360,000 to serve an unknown number of families in home visiting programs that have not been shown to reduce child maltreatment. The generic acceptance of home visiting programs as prevention against all ills appears to be part of the problem; the lack of sufficient options under the Family First Act appears to be another.
First some context. Home visiting is not a program, but rather a service delivery strategy that can be used in many different programs. There are many, many home visiting program models with different goals, services, staffing, and target populations. According to the website of the DC Home Visiting Council, the District currently offers 16 home visiting programs, each with different goals and supporting different needs. There is evidence supporting the impact of some of these programs on certain outcomes, but “home visiting” itself is neither a program nor evidence-based, despite multiple statements to the contrary at the CFSA budget oversight hearing on April 12, 2023.
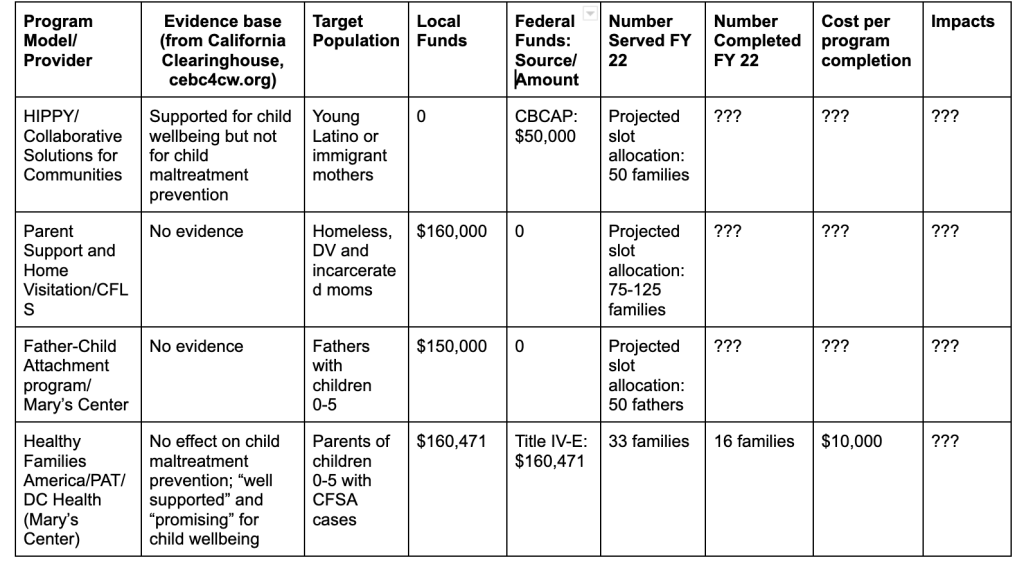
CFSA supports home visiting programs for two different populations using two different funding streams-Community-based Child Abuse Prevention Grants (CBCAP) and Title IV-E of the Social Security Act. Through CBCAP, CFSA funds three home visiting programs for “primary (universal) prevention“1 of child abuse and neglect before it occurs. CFSA uses Title IV-E funds to pay for services to families known to the agency but who may not have a substantiated allegation or an open case. These funds are transferred to the DC Department of Health (DOH) to pay for slots in two home visiting program models, Healthy Families America and Parents as Teachers, both delivered by Mary’s Center) to this population.
Programs/Clientele: In 2022, CFSA paid three providers directly for programs under CBPAP. Collaborative Solutions for Communities provided Home Instruction for Parents of Preschool Youngsters (HIPPY) to young Latino or immigrant mothers with children aged 0-6; Community Family Life Services provided “Parent Support and Home Visitation”2 to mothers who were homeless, formerly incarcerated, or affected by domestic violence; and Mary’s Center provided a “Father-Child Attachment program”2 to “fathers with children (0-5) deemed at risk.”
Evidence Base: Given the name of the funding source (Community-based Child Abuse Prevention Grants) it would be reasonable to expect that the programs funded would have evidence showing that they prevent child maltreatment. Yet, there is no evidence that any of the programs CFSA funds under this stream reduces child maltreatment. HIPPY is an education-focused program designed to prepare children for success in school and beyond. It is not listed by the California Evidence-Based Clearinghouse for Child Welfare (CEBC), the nation’s leading child welfare clearinghouse, as a home visiting program for prevention of maltreatment. Neither “Parent Support and Home Visitation” nor “Father-Child Attachment” are listed in the clearinghouse and neither appears to be a tested model. Moreover, CFSA provides no information about program outcomes in its oversight responses.
Funding: In 2022, CFSA spent $50,000 on HIPPY, $160,000 on “Parent Support and Home Visitation” and $150,000 on the “Father-Child Attachment program” of Mary’s Center.” The Mayor’s budget does not provide FY23 spending or FY24 requested funding for individual home visiting programs, or even for these programs as a group, and CFSA did not respond when I asked how much it plans to spend this year. But the testimony of DC Action for Children, which lobbies for increases in home visiting funding, suggests that the agency is planning to keep funding level for FY 24.
Number of people served: In its oversight responses, CFSA provided no information on the number of people who were actually served last year by these three programs - only the “projected slot allocation” provided in the table: 50 mothers for HIPPY, 75-125 mothers for CFLS, and 50 fathers for Mary’s Center. FY22 ended on September 30, 2022, so the agency should have been able to report on how many people were served. But CFSA Director Robert Matthews did testify that there is excess capacity in all these programs, so we can assume that fewer than the 175-225 slots allocated were filled.
The DOH programs funded by Title IV-E
Programs and Clientele: CFSA transfers Title IV-E funds to the Department of Health (DOH) in exchange for providing two home visiting programs, Parents as Teachers (PAT) and Healthy Families America (HFA), to eligible families. Potential participants include families known to CFSA but who may not have a substantiated allegation or an open case, as described in CFSA’s Title IV-E Prevention Plan. This includes families receiving services from a collaborative following a CFSA investigation or closed case; families of children who have exited foster care but are at risk of re-entry; families of children born with postive toxicology; families receiving CFSA in-home services; pregnant and parenting youth in foster care or recently exited from foster care, and their children; and siblings of children in foster care.
Evidence Base: In order to be allowable uses of Title IV-E funding, programs must have been approved as Evidence-Based Practices (EBP) by the Title IV-E Prevention Services Clearinghouse, which was created by the Family First Prevention Services Act of 2017 (“Family First”). Family First allowed Title IV-E funds, previously available only for foster care, to be used for services to prevent a child’s placement in foster care. For a program to be approved, the Clearinghouse must find that a evaluation meeting its criteria determined that the program had at least two impacts on any of seven different target outcomes.3 Unfortunately, the programs do not have to demonstrate reductions in child maltreatment, though logic suggests that such reductions would be necessary to prevent placement in foster care. Both PAT and HFA have been approved by the clearinghouse as EBP’s. But neither of these programs was found to produce meaningful reductions in child maltreatment.4One reason may be that, as evaluations have shown, home visiting programs “have struggled to enroll, engage and retain families.”
Funding: CFSA funnels $160,471 in local funds and approximately the same amount in federal TItle IV-E funds to DOH to pay for these two programs, which are delivered by Mary’s Center. According to the oversight responses, this is done through a Memorandum of Understanding (MOU) “which “pays for 40 slots of the PAT model to specifically serve the…. families defined in CFSA’s Title IV-E Prevention Plan. In addition to these 40 PAT slots, the MOU also outlines how CFSA, and DC Health will partner to ensure the child welfare agency is referring families to HFA and PAT whenever appropriate, regardless of candidate eligibility under Family First.” This is confusing. Services to families not eligible under Family First cannot legally be funded using Title IV-E so it is not clear how Title IV-E could be used to provide them.
The missing MOU: In its FY23 oversight questions to CFSA, the Facilities and Family Services Committee requested all MOU’s currently in place or planned. Those MOU’s are listed on page 148 of the Oversight Attachments. There was no CFSA-DOH MOU listed as in place as of January 23, 2023 but there was one “In Process” that dealt with “coordination around home visiting.” That is very odd, given that CFSA referred twice to an existingMOU in its responses describing the home visiting programs provided by DOH. I requested the DOH MOU from CFSA on April 21 and have received no response or explanation. Quite possibly, there is still no MOU in effect.
Numbers Servedand Cost: According to the oversight responses, CFSA referred 105 families to PAT and HFA in FY22, of whom only 33 families were served and 16 completed the programs, as shown in the table. The large dropoffs from referral to service and from service to completion are not surprising in view of CFSA Director Robert Matthews’ remarks at the budget oversight hearing. Explaining why the agency did not need more funding for home visiting, Matthews said that CFSA is not allowed to mandate participation in home visiting and that many CFSA parents do not want to participate in these programs. And it is highly plausible that the ones who do are those who need it least. At a cost of over $160,000 each in local and federal funds to serve only 33 families of whom only 16 completed the program, it looks like CFSA spent about $10,000 per program participant and $20,000 per program completer in PAT and HFA .That would be a scandal. But it is also possible that the money paid for home visiting for additional parents who were not eligible for Title IV-E funding. And that would be illegal.
Learning from the past? FY22 was not an outlier. In FY21, CFSA reported only 26 families served out of 159 referred to Mary’s Center for home visiting programs funded under Title IV-E. One might think that once CFSA saw how few of its clients were participating in FY21, they would have amended their Title IV-E plan and substituted other services for PAT and HFA. After all, CFSA said in its oversight responses that “work completed in FY22 to refer families to these services was, and will continue to be, analyzed to determine ongoing service needs for Family First target populations.” It is hard to understand how this kind of analysis would have resulted in the continuation of current funding levels for these unpopular services.
Questions and Possible Answers
Why is CFSA spending so much money on home visiting programs that are unproven to prevent child maltreatment and not popular among target families? One possible answer, most relevant to the three programs funded through CBCAP, stems from the history of home visiting. Modern home visiting was developed as a child maltreatment prevention program, and there was great hope after some initial results that appeared promising. But once the programs were rigorously evaluated, the results were disappointing. The possible exception was the Nurse Family Partnership (NFP, formally known as the Nurse Home Visiting Program). NFP was the only program shown to reduce child maltreatment using objective measures other than maternal self-reports, and it also had other impressive effects. But NFP, the only program to use nurses as home visitors, is more difficult to implement and is restricted to first-time teen mothers, and its most impressive results were achieved for White teen mothers in rural New York state. Other programs like HFA and PAT, which were easier to implement, grew more and faster, perhaps benefiting from the excitement about NFP. It was in the interests of most of the programs (and the researchers who specialized in evaluating them) to portray “home visiting” as one undifferentiated program model, allowing programs with less encouraging results to benefit from the success of their more promising peers.
One reason for the widespread use of Title IV-E funds on home visiting programs may be the lack of available alternatives. The passage of the Family First Prevention Services Act (FFPSA) in 2017 was hailed as a breakthrough for allowing the expenditure of Title IV-E funds, formerly used only for foster care, to be used for “prevention services” aimed at keeping families together. But as one essential article points out, rigid standards and administrative burdens have crippled the law’s ability to have an impact on the availability of services. Between the requirement that programs be approved by a clearinghouse as EBP’s, and the prohibition of using IV-E funds for services funded by Medicaid, jurisdictions did not have much choice (particularly in the early days of the law) if they wanted to claim federal Title IV-E dollars for “prevention services.” CFSA’s struggle to find appropriate and allowable programs that already existed in the District is made clear in its TItle IV-E Prevention Plan. Of the seven approved programs CFSA chose to implement, four were already funded by Medicaid. PAT and HFA were already being provided by DOH, which made them an attractive option for CFSA. CFSA is claiming Title IV-E funds for only three programs, two of which served only a handful of families. And CFSA is no exception. Nationwide, only 6,200 children in the whole country received a Title IV-E funded “prevention service,” for a grand total of $29 million, in FY 2022.
In light of all these concerns, I believe that CFSA should re-evaluate the home visiting programs it funds based on their effectiveness in preventing child abuse and neglect-and the likelihood that parents will choose to participate. I also believe that Title IV-E funding for HFA and PAT should be eliminated or reduced drastically. Some funds might be diverted to programs that have more recently been approved for Title IV-E funding. With the desperate need among CFSA parents for mental health and drug treatment services, CFSA should consider funneling more funds to the Department of Behavioral Health to purchase such services for its clients.
CFSA’s continued spending on home visiting regardless of purpose, numbers served, interest to families, or effectiveness in preventing maltreatment, may stem from the general misconception about home visiting as an all-purpose prevention program, as well as the lack of choices available under the Family First Act. But CFSA’s spending of Title IV-E funds in particular raises serious concerns. Not only is CFSA wasting resources but it may be diverting Title IV-E funds to an ineligible population-running the risk of having to return funds and possibly receive a penalty from the federal government. And if it is not doing that, then it is spending an unconscionable $20,000 for each person who completes the program.
Notes
While CFSA describes these programs as “primary (universal) prevention” in its oversight responses, they are actually not universal programs. Instead, they are “secondary prevention” services that target at-risk groups.
CFSA listed both these programs as “home visiting” with no program title in its oversight responses, but these program names were provided in the testimony of DC Action for Children.
The seven target outcomes are Child Safety, Child Permanency, Child Well-Being, Adult WellBeing, Access to Services, Referral to Services, and Satisfaction with Programs and Services. A program needs only two positive “contrasts” (out of as many as 80 or evem more different contrasts) between the intervention and comparison group to be approved.
The California Evidence-Based Clearinghouse for Child Welfare (CEBC), the leading child welfare clearinghouse, does not list either of these programs as Home Visiting Programs for the Prevention of Child Abuse and Neglect. The Title IV-E clearinghouse found that PAT had two very small (5% of a standard deviation), not statistically significant effects on substantiated maltreatment and neglect. The only child safety outcome for which HFA had a positive impact was self-reported (by parents) maltreatment, not a very reliable measure. In contrast, HFA had no effect on child welfare administrative reports. HFA also had no effect on any comparison of maltreatment risk assessment or medical indications of maltreatment risk.
Until recently, I was one of three “community representatives” on the District of Columbia’s Child Fatality Review Committee. Community representatives are the only members who are not paid to sit on this panel; the rest are agency representatives who sit on it as part of their jobs. My service on the panel was an important aspect of my advocacy for abused and neglected children in the District. But this work ended abruptly for me in March of this year when I was told that my service was over. As described below, I have some ideas about why the panel decided to dismiss perhaps its most engaged, passionate and productive member.
On March 2, 2023 I got a call from the Director of the Mayor’s Office of Talent and Appointments (MOTA). He said he was calling about my position on the District’s Child Fatality Review Committee (CFRC). I told him I had already received a call several weeks earlier from a MOTA staffer telling me that she was working on my reappointment, which should have happened earlier but was backlogged due to the pandemic. She asked me to submit an updated resume and told me she would be back in touch shortly to help me prepare for my DC Council confirmation hearing. But on March 2, the Director told me there had been a mistake. I was not being reappointed to the committee, and since my term had already expired, I was now off the panel.
When I asked why I was not being reappointed, I was told that it was time to give other people a chance to serve. This explanation made no sense. I was one of only three “community members” on the panel, out of eight authorized by DC Code. In her 2017 report, the DC Auditor noted the many vacant seats for community members and the importance of these community representatives, who are not tied to a specific agency. In her remarks preceding the 2017 report, CFRC Co-Chair Cynthia Wright wrote that “the addition of new community members [of which I was one] who provide a fresh perspective to our work …. has increased the vitality of the CFRC.” I doubt that there are five people lined up waiting to be appointed, or even one person ready to replace me. It’s not surprising that there is no long line of community members who want to volunteer two to four hours of their time each month in meetings about children who die, not to mention reading the sad case histories before the meetings. It was clear that my expulsion was not intended “to make room for somebody else.”
My de facto expulsion certainly did not stem from a lack of commitment or shoddy performance. I attended all 13 meetings of the Child Fatality Review Team in FY 2022 and the first quarter of FY 2023. According to the government’s responses to the oversight questions posed by the Committee on the Judiciary and Public Safety, the two other community members attended nine and seven out of 13 meetings respectively. I read every case study in advance of the meeting, and came prepared with questions and comments. Based on the questions asked at the meetings, it was clear that most members never read the case histories (sometimes as long as 20 single-spaced pages) and instead relied on the quick presentations given by Committee staff. In addition, I was a main source of new ideas on the panel; indeed, the two most recent presentations before the committee before my exit stemmed from my suggestions.1 So there must be another reason I was not reappointed. And I think I know what it is, but let me first say something about the Committee and why I joined it.
As described on the website of the Office of the Chief Medical Examiner (OCME), under which the CFRC is located, the goal of the CFRC is to “reduce the number of preventable child fatalities in the District of Columbia through identifying, evaluating, and improving programs and systems, which are responsible for protecting and serving children, and their families.” Based on the information it reviews about the histories of children who died, the CFRC makes findings and recommendations to prevent such deaths in the future. The CFRC is comprised of two teams, the Infant Mortality Review Team (IMRT), which reviews deaths of District infants from birth through twelve months, and the Child Fatality Review Team (CFRT), which reviews the deaths of children aged one to 18 years old as well as youths aged 18 through 21 who were known to the child welfare system within four years of their deaths or to the juvenile justice system within two years of their deaths.2 Their are child fatality review teams in all 50 states and some tribal nations as well.
I joined the CFRC because of my concern about children who are abused or neglected and my belief that CFRC had the potential to have a broader impact beyond preventing fatalities because the conditions that lead to child deaths also cause harm to many more children who do not die. The DC Auditor reported hearing this from several individuals who likened the fatality cases that are examined to a “canary in a coal mine.” I had a particular interest in monitoring the work of the Child and Family Services Agency (CFSA), which is charged with protecting maltreated children in the District. When I joined CFRC, I had recently left my job as a social worker at a private agency that provided foster care as part of the child welfare system led by CFSA. In that capacity, I had heard children’s lawyers express their fear that due to the recent sharp drop in removals of children from theirt homes into foster care, many were being left in dangerous situations that might eventually result in deaths or irreversible emotional or physical damage.
And indeed, upon joining CFRC, I found a number of reasons for concern about CFSA’s effectiveness in protecting children. It was astounding to learn how many children died after having some contact with CFSA. According to CFRC’s annual reports, 69 percent of families of decedents reviewed by CFRT in 2019 had prior CFSA involvement; that figure could not be calculated for IMRT reviews. Of thecases reviewed by the CFRC3 in 2020, 15 out of 18 (or 83 percent) of the decedents’ families had prior CFSA involvement. Reading the CFSA histories of these families often revealed as many as 20 reports to the hotline over the years. Many of these reports were not even accepted for investigation. Those that were investigated were often not “substantiated” or verified by the investigators, which is required for opening a case, despite what seemed like ample evidence of abuse or neglect cited in the case summaries. Even when a report was substantiated and a case was opened for in-home services, more calls often came in about the same families and investigators continued to find dangerous conditions and parenting practices. Even after the cases closed, the reports would continue to arrive, suggesting that nothing had changed as a result of CFSA’s intervention. And even when children were removed to foster care, they were often returned home with no evidence of improved parenting or conditions, and the reports continued to come in.
But when I expressed my concerns about CFSA’s response to frequently reported families and suggest that a finding or recommendation might be in order, I was repeatedly accused of “picking on” CFSA. It is as though CFSA was a child needing protection from bullying rather than an agency responsible for protecting children. Perhaps I shouldn’t be surprised. In its July 2017 report on CFRC, the DC Auditor reported this exact concern — that several panel members believed “defensive or territorial behavior remains an impediment to productive deliberations.”
It was perhaps during my second term at the CFRC, starting in 2020, that another set of issues arose that also put me outside the mainstream of CFRC members. The District was already at the forefront of a national movement to drastically reform what was described as a racist child welfare system by reducing foster care placements and government intervention in the lives of families. The murder of George Floyd and calls to abolish the police intensified this movement, with some even calling for the abolition of child welfare agencies, which were labeled as a “family policing system.” An effect of this type of thinking was an unwillingness to suggest that parents were unfit, no matter how abusive or neglectful they may have been, or to suggest that CFSA should have intervened more aggressively to protect children who later died. While my concern was for the safety of children, other members of the committee were more interested in demonstrating their opposition to governmental interference in the lives of families, regardless of the cost to children’s lives or safety.
When I joined the panel in 2017, there was more tolerance for diverse viewpoints and more concern for the needs of vulnerable children, regardless of race. There were frequent discussions about how to work with the parents who were repeatedly reported to CFSA but did not ever seem to change. Such families are well-known in the child welfare literature as “chronically neglectful,” “chronically maltreating” or “frequently reported” families. Many of these parents had problems with substance abuse, mental illness, domestic violence, or some combination of these three factors that impaired their ability to parent. They had been offered numerous services to help address these issues, which they either declined, dropped out of or completeded without any apparent benefit. Discussions of these families often led to suggestions that the agency make more use of a tool called “community papering,” which means filing a petition for court intervention to compel parental participation in services when a child is not being removed from the home. This resulted in a recommendation in the 2017 report that CFSA should use this tool more consistently for families that need some pressure to participate in services. In the same report, the panel also recommended that CFSA strengthen its policy and practice to “ensure families with multiple referrals to Child Protective Services receive an intensive historical review.” After 2017, there were no more recommendations for strengthening CFSA interventions with frequently reported families.
The changing ideological climate manifested itself in other ways. Serving on the CFRC, I soon realized that a striking number of child fatalities happen in extremely large families, with six, seven or as many as 12 children. Perhaps it is not so surprising. It’s hard to imagine safely caring for that number of children, especially if they are closely spaced. There was a time when this topic could be discussed, especially on the IMRT, whose members were concerned with protecting vulnerable infants. In the 2016 report, two paragraphs described discussion by the IMRT of “the concept of developing a public service media and marketing campaign focused on the health and economic benefits of family planning for all age ranges.” Clearly there was not enough support for this idea to result in a recommendation, but the discussion was robust enough to warrant inclusion in the report. Even in my earlier years on the Committee, this issue was occasionally raised by public health professionals. But it was no longer apparently an acceptable topic for discussion by the time my service ended in 2022.
The changing ideological climate also seemed to affect the CFRC’s willingness to address substance abuse. Parental use of alcohol, marijuana or illegal substances is a common factor cited in the cases reviewed by the panel. That includes the case of Trinity Jabore,who was born with marijuana in her system and later found dead at only seven weeks old, having suffered starvation, thirteen fractured ribs, and severe diaper rash. As the prosecutor of her parents put it, “They deliberately chose not to feed or take care of their infant and to instead smoke marijuana, PCP, get high and take selfies all day.” In 2018, the IMRT formed a subcommittee to look at the impact of marijuana usage on families in the District, in light of concerns raised by the legalization of cannabis use. In the 2019 report, the IMRT expressed concern about the role of marijuana and illicit substances in inducing a deep sleep from which parents did not rouse even as their dying babies fought for breath. But in the 2020 Annual Report, parental substance use was mentioned only in two tables and the text briefly summarizing them.
In the past, CFRC had recommended data sharing between agencies to improve coordination of services for the most troubled families, who are often involved with multiple agencies. In its 2016 report, reflecting the period just before I joined the panel, the CFRC recommended that the District “should allocate funding for the implementation and utilization of DC Cross Connect throughout the human services and public services cluster agencies” in order to better meet the needs of vulnerable children and families. (The recommendation was directed to the Department of Human Services (DHS), which did not have jurisdiction over the other agencies included in the recommendation, and DHS did not respond to that part of the recommendation.) Cross-Connect is an effort to integrate care between DHS, the Department of Behavioral Health, and CFSA, incuding the sharing of data. In 2022, I became aware that a similar proposal for a citywide database to track information on anyone served by DC government agencies is a key element of the Gun Violence Reduction Strategic Plan prepared for the District by the National Institute for Criminal Justice Reform, and I suggested that we might consider such a recommendation. My suggestion resulted in a presentation by the CJCC but not a new recommendation for sharing data between agencies in the District. This new ideological climate, where there is great suspicion that data sharing can be used against marginalized populations, rather than to protect their most vulnerable members, was not fertile soil for such a recommendation.
It is unfortunate that I cannot relate specific details behind the generalities that I have reported here, except those taken from published annual reports. Strict rules around the confidentiality of meetings and information shared govern the operations of CFRC. Before every meeting, members sign a confidentiality agreement promising not to disclose any information discussed during the meeting. Those rules are clearly excessive. The panel is given case histories with no names provided. These case studies can and should be available to the public (with the redaction of any information that could give away the identity of the families.) The public deserves to know that the funds it spends on child protection often fails to protection children. Hiding this information merely protects the agencies involved. That’s why I’m hoping that the DC Council will pass legislation allowing the release of the summaries provided to CFRC (with redaction of any information that would clearly give away the identity of the decedents and their families.)
In his preface to the CFRC’s 2018 report, Chief Medical Examiner Roger Mitchell stated that “the CFRC is moving toward being a leading voice in the prevention of child fatalities in the District of Columbia.” But until committee members are willing to put the needs of children first, CFRC will never be such a leading voice in preventing child fatalities in the District. Now that I am off the CFRC, I hope that other members will be courageous enough to stand up for the rights of children to be safe and well cared for, even at the risk of becoming a gadfly-which was clearly the reason for my removal.
Notes
These presentations focused on: (a) Criminal Justice Coordination Committee on DC’s Gun Violence Prevention Plan and its work to implement it; and (b) the US Attorney’s ATTEND program to reduce school truancy.
There was no on-boarding or training when I entered the pane, so it took me at least a year to realize that I was eligible to join the IMRT as well as the CFRT. Once I understood that CFRC members are eligible to participate on both teams, I began attending the IMRT meetings as well.
This includes only those cases reviewed in full by the IMRT; this information was not available for those that were included only as part of a statistical review, which is used as a way of studying the deaths of most infants who died of natural causes. Many IMR cases are reviewed statistically not individually; for example 14 out of the 51 cases reviewed in 2019, (the last normal year before Covid) were reviewed statistically. In 2020, during which the committee missed six months of case reviews, 29 of the 47 cases reviewed were statistical reviews of infant natural deaths.
CFSA’s newest Child Fatality Review Report focuses on the deaths of 29 children and young adults whose families were known to CFSA within five years of their deaths and whose cases were reviewed in 2021. This report’s toll includes one mother who lost two little children in one year-one who died of fentanyl poisoning and another left alone with a four-year-old sibling and a propped bottle. It included four overdose deaths from synthetic opioids and ten “non-abuse” homicides including the shooting of a six-year-old at 11pm outside a liquor store. It included a twelve-year-old who died of an untreated bacterial infection but had signs of abuse on her body. Most of the dead children’s families had been reported to CFSA at least four times in the past five years. Many of them had experienced investigations and received CFSA-supervised services. Nevertheless, these children died within five years of their contact with CFSA. But the agency’s child fatality reviewers made no recommendations to improve screening, investigation, or services. That is not a surprise, given the agency’s current tendency to minimize intervention in the lives of troubled families.
When a child known to a child welfare agency dies, a natural question is whether the agency could have prevented that death if it had done more or different things. For that reason, fatality review is an important way to assess the performance of a child welfare agency, both internally and externally. According to an appendix to the report, the mission of the CFSA Child Fatality Review (CFR) Unit is “to reduce the number of preventable child fatalities in the District of Columbia through identifying, evaluating, and improving programs and systems responsible for protecting and serving children and their families.” CFSA’s 17th annual Child Fatality Review Report, based on the work of the CFR Unit, was released on January 30, 2023.1
Before 2019, CFSA followed the common practice of including in a given year’s CFR report all of the fatalities it reviewed during that year, even if they occurred during previous years. This makes sense as these deaths were never discussed in earlier reports. But for the third year in a row, CFSA chose to eliminate some cases from its analysis based on when they occurred. The new CFR report includes only those deaths that occurred during 2021 and were reviewed in the same year. That means their analysis includes only 29 child fatalities instead of the total of 51 fatalities they actually reviewed in 2021. The rest of those fatalities occurred in 2018, 2019, and 2020. See the Note on Timing appended to this commentary for further discussion of this issue.
Manner of Death
The manners of death2 of the 29 young people whose cases are included in the body of the report are displayed in the pie chart below. About a third of these decedents were victims of “non-abuse homicide;” six (or 21 percent) died of accidents; four (or 14 percent) died of natural causes; and three (or 10 percent) died of “neglect homicide.” The other six children’s manners of death were “undetermined” or “unknown.”
Three, or 10 percent of the deaths reviewed in this report, were labeled as “neglect homicides.”(There were no homicides attributed to abuse). All of the victims were age three or under, which is typical of child maltreatment fatalities nationally as well. One of the three was a 17-month-old with “thermal and scald” injuries. The two other fatalities both involved synthetic opioid toxicity, illustrating the spread of this crisis to the District of Columbia. The second fatality was a three-month-old who died of synthetic opioid (eutylone and fentanyl) toxicity and the third was a three-year-old boy dead of fentanyl toxicity.The families of the 17-month-old and the three-year-old both had more than ten hotline calls and had open in-home cases at the time of the fatality.
Non-abuse homicide
By far the most common manner of death reviewed in this report was “non-abuse homicide,” or homicide that was not the result of child abuse. Such “non-abuse homicides” were one-third of all deaths reviewed; eight of the decedents were male and two were female. One victim was only six years old; the remainder were aged 13 and older. Nine of these deaths were caused by gunshot wounds and one was caused by stab wounds. One of the victims was in foster care with a relative at the time of his death. He had been removed from his home in 2015 due to abuse and neglect.
Natural Causes
Three fatalities, or 10 percent of the deaths included in the report, were due to natural causes. All of these children had congenital anomalies. They included a four-day-old girl and a three-year old boy who were both born prematurely and were medically fragile. Both of their families had open cases with CFSA. The three-year-old had been placed with a foster parent experienced in caring for medically fragile children after his mother was determined to have neglected him and was determined to be ill-equipped to care for a medically fragile child.
Accidental Deaths/Unsafe Sleep:
The manner of death was deemed to be accidental for six, or 21 percent of the deaths reviewed. Unsafe sleeping arrangements were involved in three of these six deaths of babies whose ages ranged from 19 days to two months old. In all of these cases, asphyxia was included as a cause of death. Of the remaining accidental deaths, two girls aged 16 and 17 died of opioid overdoses. Both deaths were part of a spate of fatalities in June 2021 that the police attributed to a tainted batch of fentanyl. The final accidental death was that of a four-year-old child who was hit by a car. An observer reported that he wandered away from his mother and two younger siblings before being hit.
Undetermined and unknown
Four of the fatalities were classified as undetermined because the autopsy findings were inconclusive. In one case, the mother left an 11-month-old and her four-year-old sibling sleeping alone in the home, and returned to find the baby unresponsive and foaming at the mouth. In a re-enactment using a doll, the mother demonstrated placing the child on her stomach with a bottle in her mouth in a way that could have impeded her breathing, but the medical examiner was unable to confirm asphyxia as a cause of the baby’s death. In the wake of the fatality, CFSA opened an in-home case to help the mother and her children. But that was not enough to save her three-year-old, who died within six months of opioid toxicity while the in-home case was still open, and was one of the three neglect homicide victims mentioned above. Unsafe sleep environments were involved in two of the other deaths for which the manner was undetermined.
The fourth death for which the manner was undetermined involved a twelve-year-old girl who reportedly collapsed after choking while eating soup. However, the hospital physician observed bruising on the child’s abdomen, back and legs, the mother was found to have abused her, and two siblings were removed from the home. The official cause of death was an untreated bacterial infection coupled with pneumonia but the manner could not be determined.
There were three deaths for which the manners were unknown. A seven-week old boy was reported missing by his father and is presumed dead. The mother was charged with suspected concealment or removal of the body and her other three children were removed from her. Unless there were two babies close to two months old who were reported missing in 2021 under the same circumstances, this is a case that received considerable media attention. The mother told the baby’s father that he had been removed by CFSA. Eventually she told police that she accidentally rolled over her son while under the influence of PCP, then panicked and threw his body into the trash. She was initially charged with murder but the charges were dropped as a body was never discovered. According to police, the mother was stabbed to death by the father in April 2022.
The remaining deaths for which the manner is unknown involved a newborn removed by Caesarian from a mother dying of Covid-19 and a seven-year-old who died in a house fire, for whom autopsy results are pending.
Decedents in Foster Care at TIme of Death
Two of the decedents were in foster care at the time they died. One was the eighteen-year-old who was living with a relative after being removed from his abusive mother, and who was the victim of a non-abuse gun violence homicide. The other victim was the medically fragile two-year-old, who was dependent on a gastrostomy tube and a tracheostomy vent, who died of natural causes and was living with a foster parent who specialized in caring for medically fragile children.
Family Risk Factors
The report provides some demographic information about the parents of the children who died, and that information is in line with research evidence that teen parenting, large families, and a parent’s history of maltreatment as a child are risk factors for child maltreatment. Parents of the children who died tended to be very young when they started having children. Sixty-nine percent of the mothers and 58 percent of the fathers were under age 21 at the birth of their first child. The youngest mother was 13 years old when she gave birth to her first child and the two youngest fathers were 16. Many of the dead children came from large families, which is more common among those who start having children at an early age. All but four of the 29 decedents had two or more siblings. Thirteen had four or more siblings; three had seven or more siblings, including two with 12 siblings and one with 10 siblings. A parent’s maltreatment history as a child is also known to be a risk factor; 13 of the 29 birth mothers had CFSA involvement as children, and both parents of two of the decedents were involved with CFSA involvement in their childhood.
Parents’ CFSA History as Caregivers
Nine of the 29 families reviewed in the report (or about a third) were involved with CFSA at the time of the fatality. Of these nine families, two had an open investigation and five had an open in-home case. Two had an open foster care case, but those are presumably the families of the two children who died while in foster care.
Table 7 shows that 10 families (or more than a third of the 29 families) had CFSA involvement within 12 months of the fatality - only one more family than was involved at the time of the fatality. It appears that all of them had an investigation within that period. However, with fewer families reported to have an in-home or foster care case than in Table 6, there must be some errors in the data; CFSA has not yet responded to a request for clarification.3
Looking at the 17 families that did not have CFSA involvement at the time of the fatality (Figure K in the report)4 CFSA found that the time since they were involved varied from 1 to 56 months, and that 11 of these 17 families (65 percent) were last involved with CFSA more than 18 months before the fatality.
As shown in Figure J, the majority of the families had four or more reports to the hotline (known as referrals) during the five years preceding the fatality. Many of these reports were screened out, as shown in Figure Q. All but 4 of the 29 families had referrals that were screened out during the five-year-review period and ten of those families had five or more referrals screened out.
Table 8 summarizes the results of the reports received regarding these families. The large majority of these families (23 families or 79 percent of families) were investigated at least once , with an additional 6 families investigated twice. Twelve families (41 percent of families) had in-home cases within five years of the fatalities, with eight having one case, three having two cases, and one having three cases.5,6
Figure L in the report (not reproduced here) shows that 16 families, or slightly more than half of the families, had at least one substantiated allegation in the five years before the fatality. Ten of these families had only one substantiation and the remaining families had between one and four substantiated allegations. The most common substantiated allegations were inadequate supervision and educational neglect (four families each), followed by physical abuse, failure to protect, medical neglect and indadequate food/clothing/hygiene (three families each).
“4+ Staffings“
One CFSA practice that is designed to prevent further harm to children known to the system is the “4+ Staffing.” CFSA conducts these meetings for families that have four or more referrals, with the last referral occurring within the past 12 months. These staffings are supposed to uncover gaps in past practice or service delivery that may have contributed to the repeated maltreatment and to find strategies to prevent future maltreatment. In the 2020 CFR report, CFSA stated that of the decedents’ families who had qualified for such a staffing during the five years before the fatality, all had received a 4+ Staffing. Clearly, this figure casts doubt on the effectiveness of these staffings. Unfortunately, the analogous section of the current report appears to focus on the percentage of eligible families that received a 4+ staffing after the fatality, a fact that is less relevant to the purpose of CFR.7
Siblings removed after child fatalities
A new report section states that 11 children were removed from four families in the wake of the child fatalities reviewed in the report.
After an 11-month old girl was left alone with a four-year-old sibling and a propped bottle, the agency opened an in-home case for the family. But when her three-year old brother died of fentanyl intoxication within six months of his sister’s death, the other children were removed and placed with kin. At the time of the writing of the report, their goal was reunification with the parent, who was said to be “receiving services, including grief counseling for the loss of more than one child within a short time frame, as well as substance use and housing.”
The siblings of the 12-year-old girl who died of an untreated bacterial infection but also had signs of physical abuse have already been returned home. CFSA states that the mother and children have received mental health services and the mother has completed court-ordered parenting education.
Of the three siblings of the infant boy who disappeared, one child was with her father at the time of the report’s being written and the other two were placed in foster care with a goal of reunification.7
The 17-month-old who was scalded to death had four siblings, ranging in age from five months to twelve years old, who were all removed from the mother in the aftermath of the toddler’s death. Two were placed with kin and two in a mysteriously named “non-foster care placement,” which probably connotes placement with kin outside the foster care system. There is no mention of reunification; perhaps this case qualified for the exemption from reunification that is allowed under certain aggravated circumstances.8
CFSA’s Findingsand Recommendations
In its Summary of Critical Findings, the CFR report discusses specific areas that received “additional focus” in 2021, including screened-out referrals. Concerns about the accuracy of hotline decision-making have been expressed in the District and around the country. In a 2016 study, conducted by the Center for the Study of Social Policy, the court monitor in the LaShawn class action suit, reviewers disagreed with CFSA’s decision to screen out the referral in 27 percent of the referrals studied. However, the report does not suggest any review of policy or practice in screening out referrals. Instead, it cites the “prevention services” provided by the collaboratives and the family success centers. The report also devoted special focus to families involved with CFSA at the time of the fatality, unsafe sleep fatalities, and gun violence, but the report makes no suggestions about how to avoid such fatalities involving these factors.
Based on its fatality reviews, CFSA’s ICFR Committee approved three recommendations: revision of the critical event and child fatality review policies, integration of child fatality review data into the new computerized case management database currently being developed, and finalizing a Memorandum of Understanding with DC Health “to provide monthly data on applicable fatalities to CFSA to facilitate the timely review of child fatalities.” It is notable that all these recommendations address the child fatality review process itself. There are no recommendations for changes in policy or practice related to screening, investigations, or services. It is also significant that the following language about the purpose of ICFR recommendations which was included in the 2020 report does not appear in this one: “The CFSA ICFR committee makes recommendations concerning appropriate actions that may possibly avert future fatalities.” Perhaps this language was deleted because none of this year’s recommendations are aimed at averting future fatalities, just about amending the fatality review process.
Conclusions
It is important to remember why we study child fatalities. These tragic deaths are the tip of an iceberg - the visible consequence of recurring abuse and neglect after at least one incident of alleged maltreatment was reported to the agency. When a child remains in the home after services end, we may not know that maltreatment has continued unless the child dies. Some children known to CFSA die for causes that are not related to abuse and neglect, like the newborn delivered early from the mother dying of COVID-19, or the three children with congenital abnormalities who died of natural causes. But research shows that simply having a report of child maltreatment increases the risk of deaths from all causes, not just abuse or neglect. Thus, many of the fatalities included in the report may be a consequence of ongoing maltreatment, even if the manner of death was not found to be maltreatment.
Some of the deaths with a manner labeled as accidental or unknown may have been due to neglect, like some of the eight babies who died while sleeping in unsafe arrangements. In total, CFSA reported that unsafe sleep factors were present in eight of the 10 deaths to children aged two or under. In my years of service on the citywide Child Fatality Review Committee,1 I have seen numerous cases of children dying in unsafe sleep environments in families with histories of child welfare involvement. Almost invariably, the parents have used marijuana, alcohol or other intoxicants before lying down with the baby, and they failed to wake up as their children struggled to breathe. With unimpaired parents, these sleeping arrangements might not result in death. This is why a study found that adjusting for risk factors at birth (including low birth weight and late or absent prenatal care), the rate of Sudden Unexplained Infant Death (SUID) was more than three times greater among infants who had been previously reported for past maltreatment than among infants who had not been reported.
And then there are the ten deaths from “non-abuse homicide.” The connection between child maltreatment and violent death became obvious to me soon after I started sitting on the citywide Child Fatality Review Committee. I learned that many young victims of homicide grew up in families with long histories of reports to CFSA regarding lack of supervision, school absences, physical abuse and other concerns. In some cases CFSA screened out the reports or found no maltreatment; in other cases services were provided. But the maltreatment continued. Many of these families exhibited chronic child neglect, which occurs “when a caregiver repeatedly fails to meet a child’s basic physical, developmental, and/or emotional needs over time.” Many of these children, with histories of trauma and little support at home or connection to school, eventually found belonging in the streets and took up violent and illegal activities.
Of course, we do not know how many of the gun violence victims included in this report came from abusive or neglectful homes or were involved in violence themselves. But according to police reports, motives for five of the nine homicides included retaliation for robbery and gang-related activities, implying the victims were involved with such activities. Relatives of the 18-year-old female victim of another homicide indicated that she was involved in a “volatile” relationship with her killer. The six-year-old whose death is reviewed here was obviously an innocent bystander. But she was shot while walking to a liquor store with her parents late on a Friday night. And federal prosecutors stated that the father of the six-year-old shot on July 16, 2021 was involved in the violent drug trade on the street where his daughter was shot, and the judge indicated that he did not understand what the child was doing in that area at 11:00 PM.
The four-year-old who was hit by a car when he wandered away from his mother might also be a victim of neglect, but we do not know because no case details are provided in this report. And as for the teenage girls dead from tainted fentanyl, we will never know what kind of home environment they had and if that contributed to their drug use. But the connection between childhood maltreatment and later substance abuse is well-known.
Of course CFSA understands the linkage between abuse and neglect and all causes of death. That’s why it studies all deaths of children known in the past five years, not just those due to maltreatment. CFSA had many opportunities to intervene in the lives of the 29 children discussed in the report and their families. Nine of the families were involved with CFSA at the time of the fatality. Ten of the families were involved with CFSA within a year of the fatality. Within five years of the fatality, 25 of the families had at least one screened-out report, 23 of the families had at least one investigation, and 12 of the families had at least one in-home case.
Obviously it is concerning that two fatalities occurred in families that were being investigated by CFSA and five occurred in families that had an open in-home case, In which a CFSA worker is expected to visit a family from weekly or twice a month, depending on its perceived need. One has to wonder whether any red flags were missed by the workers who were investigating or monitoring these families. Among the families that had an open in-home case at the time of the fatality were the families of both the 17-month-old and the three-year-old who died of synthetic opioid toxicity. One cannot help wondering how frequently and thoroughly the in-home workers interacted with the families, without noticing that the parents were still using opioids. Nobody wants to remove more children, but perhaps they needed to be removed, and some of these children may have had a protective relative ready and eager to receive them.
I do not mean to say that CFSA could have saved all of the children that they touched who later died. But perhaps it could have prevented some of these deaths. The agency could have chosen to devote special attention to parents who were very young when they started childbearing, families with many children, and parents who were involved with CFSA as children. It could have screened in more referrals, substantiated more allegations, opened more cases, monitored families more effectively, provided more intensive and effective services, or involved the court in more in-home cases. And if necessary it could have removed more children, preferably to a protective relative or other known adult.
The total of 29 children who were known by the end of 2021 to have died after being touched in some way by CFSA will certainly rise as more fatalities are identified and reviewed. (The total for 2020 is 40 so far.) But if present practices continue, the remaining fatalities will not be included in an annual report, except for one or two tables in the appendix. Therefore, the annual reports understate the number of children who died after being touched by CFSA. Strangely, the report authors do not seem to understand the significance of the smaller universe, making comments like “There was a decrease in total infant fatalities in 2021.” That decrease, from 16 to 10, may not mean much when the total number of fatalities reviewed was 29 instead of 40.
It is concerning that all of the report’s recommendations concern the practice of fatality review itself. There are no recommendations to improve CFSA’s practice in conducting the hotline, investigations and in-home and foster care cases. It is hard to avoid thinking that CFSA’s ideology of non-intervention and family preservation has contributed to both these deaths and the lack of recommendations aimed at preventing such deaths in the future. No child welfare agency has a crystal ball. They all have to strike a balance between the harms caused by intervening in families where there is no maltreatment and not intervening in maltreating families. But CFSA has declared its preference clearly. As stated in the report, “For over a decade, CFSA has invested in safely keeping families together and developing robust prevention strategies to help support them.” But these “robust prevention strategies” were not enough to protect the children who died in 2021. For CFSA, these deaths may simply be collateral damage.
The information about the siblings who were removed from their families after the fatalities - a new addition to the report - is quite disturbing. The idea that the agency is still working for reunification with the mother who lost two children in one year - one left alone with a four-year-old and a propped bottle and the other poisoned by fentanyl - and had ten hotline reports in the five preceding years is concerning. And that the siblings of the abused child who died of a bacterial infection are back with their mother after she received mental health services and parenting education is concerning as well. But it is not clear what CFSA could have done differently without action from the DC Council. The DC Code requires CFSA to make “reasonable efforts” to reunify children with their families except in certain aggravating circumstances which probably would not have been found in these cases.9
As always, CFSA’sinternal child fatality report is distressing. It includes two deaths in one year to the same family, ten non-abuse homicides, several deaths involving unsafe sleep, and two high-profile child deaths: an infant whose body was disposed of by the mother and a six-year-old who was killed as part of a drug war involving her father. We learned of four deaths - two of small children and two of teenagers - involving the new scourge of fentanyl and other synthetic opioids. CFSA has made the decision to avoid intervention and prioritize family preservation above child safety, and the report contains no recommendations for improving the agency’s efforts to spot and address abuse and neglect. If CFSA is not going to make any recommendations to protect children in the CFR report, then one might question the report’s purpose and utility.
Notes
It is important to distinguish CFSA’s internal child fatality reports from the annual reports of the citywide Child Fatality Review Team, which covers all deaths of young people up to age 18 and some deaths of those aged 19-21.
‘Manner of death” refers to the circumstances that caused the death, as opposed to “cause of death,” which refers to the specific disease or injury that led to the death.
It is also unclear why only one child is counted as having a foster care case since two of the children were in care at time of death.
This count of 17 families that did not have CFSA involvement at the time of the fatality is inconsistent with Table 6 and the associated text, which says that 20 families did not have active CFSA involvement at the time of the fatality.
The heading “Reports” in this table is confusing but I have followed the lead of CFSA in describing the Table’s data and am awaiting clarification from the agency.
Family assessments were an alternative to an investigation for low-risk cases, and are no longer being used by CFSA.
I have asked CFSA to clarify the meaning of their data on families that received a 4+ staffing but have not received an answer as of the date of this publication.
If this is indeed the case referred to earlier, this reunification will not take place as the mother has been killed by the baby’s father. It is possible that the oldest daughter’s father is a different person and that she can remain with him.
Until 2019, CFSA’s internal child fatality reports covered the agency’s reviews of all fatalities of children whose families were known to the agency within five years of their death. This is normal for child fatality review panels, which often have a long time lag before reviewing a case. But in 2019, ICFR decided to include in its review only the deaths that actually occurred in the year they were reviewed. As I have described, one problem with that approach is that it is clearly impossible to review all deaths that occurred in a given calendar year during that same year. Deaths that occur or become known near the end of the year clearly cannot be reviewed during that same year. Perhaps as a result of that realization, the CFR Unit included in the 2020 child fatality report those child deaths that occurred in 2020 and were reviewed during the same year or in the first three months of CY 2021. That decision gave them a total of 40 cases that were included in the report. However, this year, CFSA, as in 2019, including only the cases reviewed during the calendar year, missing any cases that were reviewed in the first quarter of 2022 or later. This is particularly strange because this report was released so much later than the last report with respect to the calendar year reported on - January 2023 as opposed to October 2021. So they had more time, not less, to include an extra quarter of reviews.
There is another problem with limiting reviews to the current calendar year, which is that deaths occurring in earlier years are missed. In Appendix A and B, the ICFR reports that it actually reviewed 51 deaths in 2021. Thirteen of these deaths occurred in CY 2020 and were apparently reviewed in the first quarter of 2021 and included in the 2020 report. However another 14 fatalities that occurred during 2018 and 2019 were presented to the ICFR committee during 2021 but not included in the report. These fatalities were never included in previous analyses, nor will they be included in the future, so most of the information on these fatalities will never be released to the public, aside from some demographic and cause and manner of death data provided in Appendix C.
There is also an internal inconsistency between the 2021 report and the appendices. The report contains reviews of 29 cases. Appendix A states that “the ICFR Committee reviewed 51 fatalities during CY 2021; all 51 fatalities helped to inform practice and policy recommendations that potentially reduce future child fatalities.” It states that 13 of these fatalities occurred in 2020 and were included in the previous report, and another 14 of these fatalities occurred in 2018 and 2019. That means that out of the 51 fatalities reviewed in 2021, only 24 (51 minus 27) occurred in 2021. Yet, the 2021 analysis includes 29 fatalities. I have asked CFSA about the discrepancy but have not received an answer as of the date of publishing this commentary.
Good morning! Thank you for the opportunity to testify today. My name is Marie Cohen and I write the blogs Child Welfare Monitor and Child Welfare Monitor DC. After my first career as a policy analyst and researcher, I became a social worker and served in the District’s child welfare system until 2015. Soon after leaving that job, I began writing these blogs to share some of the insights I had gained from my time in the field, and I’ve been amazed to see both of my blogs acquiring readers and influence beyond my wildest dreams. I take a child-centered approach, placing the safety and wellbeing of the child above all other considerations. I also take a particular interest in translating academic research for a lay audience and exposing misinterpretations of research by those trying to support their point of view. In my testimony today, I’ll start by talking about CFSA’s performance in child protective services, then continue with in-home services and then foster care. In conclusion, I’ll explain why I fear that CFSA is losing interest in these core services in its desire to become a “child and family well-being agency” and why I hope that the Council will encourage a renewed focus on CFSA’s primary mission.
My testimony draws from several sources. First, I have used recent CFSA reports including the FY 2021 Needs Assessmentand the performance oversight responses recently submitted to the Committee, as well as the CFSA Data Dashboard. I also share some insights from my service on the Child Fatality Review Committee and as a mentor through BEST Kids for almost seven years. Finally, I draw from the national research and policy trends I that I review for my blog.
CFSA has had some successes in the past year. The agency has returned to a mostly normal service posture after the pandemic-induced transition to virtual services. It has found a creative way to claim federal funds for case management and improved one service for families with substance abuse by bringing it in-house. The agency is increasing the number of professional foster parents, though not by enough so far, and the menu of therapeutic services available to foster youths and their parents through a contract with MBI. It has used federal funds to add four new staff members to work with schools and families to reduce school absences due to educational neglect. But CFSA is still falling short on meeting its primary missions of keeping District children safe and providing a physically and emotionally safe haven for those children who must be removed from their homes.
Child Protective Services: CFSA’s primary mission of protecting children has suffered as the agency has continued to emphasize narrowing the front door.
CFSA often boasts about the drop in the foster care rolls, which have fallen from over 1500 on September 30, 2012 to only 614 on September 30, 2021, crediting its policy pillar of “Narrowing the Front Door.” But a drop in foster care numbers is not in itself a positive outcome unless it has been achieved without compromising the safety of children. The choice of “Narrowing the Front Door” rather than “Keeping Children Safe” as the first pillar is not accidental: the goal has become reducing foster care regardless of the impact on child safety. Moreover, CFSA is no longer serving more children in their homes as they place fewer children in foster care; the number of children receiving in-home services has also fallen since 2019, with the total number of children served decreasing from 1994 at the end of FY 2020 to 1904 at the end of FY 2021.
My service on the Child Fatality Review Committee (on which I am thankful to have been joined by Chairperson Nadeau), has revealed many occasions in which CFSA missed chances to protect some of our most at-risk children. I have reviewed death after death of children from families that were the subject of multiple reports to the CFSA hotline dating back many years. Yet these allegations were repeatedly screened out or not substantiated by the agency. CFSA needs to assess the operations of its hotline and investigations, which have both been criticized by the Court Monitor in the past, to make sure that its desire to narrow the front door is not outweighing the concern for child safety. But there is also something the Council can do. I have noticed that many children who later died were at some point assessed to be at high risk but were left after an investigation with no support or monitoring by CFSA. When I ask why, I am reminded that CFSA cannot open a case if abuse or neglect was not substantiated, no matter how risky the situation appears to be. So whether we can protect a child depends on whether harm has already occurred, not whether it is likely to occur. But not all jurisdictions require substantiation in order to open a case for in-home services or foster care. In Washington State, an allegation does not need to be substantiated for an agency to file a neglect petition in court; the purpose of filing a petition is to “prevent harm” and there is no need to prove that harm already occurred. In Michigan and Minnesota, a case can be opened or a child removed because of “threatened harm,” which can be substantiated as a type of maltreatment. I hope the Council will consider changing DC law to make it possible for CFSA to protect at-risk children before it is too late, even without a substantiated allegation.
In-home services: Services provided through CFSA’s Prevention Services Plan are reaching few people and wasting funds, at the same time as CFSA is failing to provide families with needed behavioral health and other services.
The Family First Prevention Services Act allows CFSA to spend Title IV-E funds for evidence-based family preservation or reunification services to prevent entry or re-entry to foster care. However, only evidence-based practices (EBP) that are approved by the Children’s Bureau’s Prevention Services Clearinghouse can receive federal reimbursement. Currently, the only services receiving Title IV-E funding from HHS are Motivational Interviewing, which is part of CFSA’s case management model, and a home visiting program called Parents as Teachers (PAT) that is run by the Health Department. The other services included in CFSA’s Prevention Plan are funded by Medicaid or other local sources.
CFSA deserves credit for realizing that one practice that is reimbursable under Family First, motivational interviewing, could be incorporated into case management, thus allowing CFSA to collect matching funds for case management for all families receiving services in their homes. This was a creative way to claiming federal funds despite the flaws of the Family First Act, under which has not brought about the promised bonanza of federal resources for family preservation services. I also applaud the agency for improving the performance of Project Connect since they brought the program in-house. Project Connect provides intensive home-based services to families with an in-home case who are addressing substance abuse. When provided by a contractor, Project Connect struggled to enroll families, but now that it is operated by CFSA, the agency reports that the program has been at capacity since January 2020. The agency reports 46 families served, and 26 cases closed, with 9 families having disengaged and 17 having completed the program in FY 2021. Of course the longer-term outcomes of the program in terms of sobriety and child maltreatment remain to be seen and I hope CFSA will be reporting on them.
But the other services provided in CFSA’s Prevention Services Plan are reaching few people. According to the FY 2021 Needs Assessment, only 8% of the families referred to DBH received services. Similarly, only 8% of clients referred to the Department of Health home visiting programs, Parents as Teachers and Healthy Families America (HFA, the other DOH-run home-visiting program,) received services. Most of these referrals were either rejected as not appropriate or withdrawn because the family did not engage. According to CFSA’s oversight responses, CFSA referred 159 families to Mary’s Center for home visiting services through the HFA and PAT models in FY 2021, but only 26 of these families were served. CFSA paid over $160,000 to Mary’s Center to provide PAT in 2021; we don’t know how many of the 26 families received PAT or completed the program, since data on PAT and HFA are combined. Several other programs included in the prevention plan served between 0 and 4 families, according to the oversight responses.
At the same time as CFSA was paying $160,000 to enroll 26 families in PAT, parents and children who wanted basic behavioral health services such as cognitive-behavioral therapy and medication management could not get them because of the crisis in the District’s mental health system that affects all residents who must rely on Medicaid to access services. I hope the Council addresses this crisis. But regardless, there is no gain in accessing federal money to serve no-one. CFSA might as well spend this money on services families need, whether or not they are approved for Title IV-E funding.
Another set of services that is sorely needed for CFSA families are services to address domestic violence. According to CFSA’s 2021 Needs Assessment, of 123 child welfare professionals, the largest percentage (64%) ranked domestic violence (DV) as a prevalent risk factor among their clients. It is encouraging that the 2021 Quality Services Reviewers found three-quarters of the families with DV in in-home cases were receiving services. But some of these services were provided by the CFSA social worker themselves, presumably because services were not available. Moreover, the reviewers found that accessing the agency’s one DV specialist for consultation was a challenge for social workers and that case managers for only six of the 16 families reviewed were able to obtain such a consultation. I hope that the Committee will choose to add funding for at least one more DV specialist to make sure that caseworkers can benefit from a real expert to determine what their clients need and link them with services. The Needs Assessment also indicates that there is a general shortage of DV services in the District, which I hope the Council will address.
Early care and education is one service which has great potential to prevent maltreatment recurrence among families with in-home cases, but has been largely ignored by CFSA. Guaranteeing a slot in a high-quality preschool like Educare in Ward 7 for every preschool-aged child involved in an in-home case might do more to prevent child abuse and neglect than any other single strategy. We know that high-quality early care and education prevents child abuse and neglect by multiple pathways: easing parental stress, providing family support and parenting education, increasing monitoring by mandatory reporters (at Educare children are checked for abuse daily), and simply reducing the amount of time a child is alone with caregivers and vulnerable to abuse. And indeed, multiple studies link early care and education with reductions in child maltreatment. I hope the Committee will work with CFSA, the Mayor and OSSE to ensure that all children with in-home cases receive high-quality early care and education.
Foster care is not yet a truly safe haven where youth in CFSA custody can heal from past trauma and address educational deficits.
When CFSA takes the drastic step of removing a child from their home, it has the obligation to make sure the child is placed together with siblings, in the home of either a known relative or family friend if possible, and with all the necessary supports, including mental health services, the best healthcare (including covid-19 vaccines) and educational and vocational supports. And whenever reunification is not possible, CFSA should stop at nothing to support permanency with real or fictive kin. But CFSA is falling short in these areas. Often agency leaders seem to lack the creativity, passion, and outside-the-box thinking that is necessary to make foster care the safe haven that CFSA advertises.
Foster care: CFSA continues to lack appropriate placements for older youth and those with significant behavioral health needs.
The lack of suitable placements for older youth and those with more serious behavioral health needs continues to be a crisis leading to placement disruptions, abscondence, and further deterioration in the mental health of our most vulnerable youth. This issue has been covered in depth the Children’s Law Center in their written testimony. In general, I agree with their findings and recommendations on building an adequate placement array but I would add that CFSA may have to consider adding one or more therapeutic group homes as well as increasing its supply of professional foster parents. There are simply not many potential foster parents who are dedicated and gifted enough to take on these very challenging young people.
Too few foster youth are receiving the behavioral health services they need.
Only 18 children were receiving therapy at CFSA in the first quarter of FY 2022, out of the 600+ children in foster care, according to CFSA’s oversight responses. That means CFSA’s four in-house therapists are being paid to provide therapy to only 18 children, so that each therapist is seeing fewer than five children a week. CFSA did not report on the number of children receiving therapy outside of the agency, but the low number receiving in-house therapy is concerning. Moreover, according to the 2021 Needs Assessment, the percentage of children recommended for therapy who received it went down from 69% in FY 2020 to 40% in the first half of FY 2021. I understand there is a citywide crisis in mental health services, with a catastrophic shortage of providers, not to mention quality, cultural competence and turnover, as the Children’s Law Center explains in its written testimony. I join the CLC in urging that this Committee work with the Committee on Health and the rest of the Council to fix the District’s behavioral health system. However, until this reform can take place, CFSA must not waste the resources it has allocated for behavioral health for its foster care youth.
I do appreciate, however, that CFSA has added two popular evidence-based therapeutic modalities – Dialectical Behavior Therapy (DBT) and Eye Movement Rapid Desensitization Therapy (EMDR) - through its contract with MBI Health. And I’m also happy that CFSA has included parents of children in foster care in its contract with MBI. However, I’m disappointed that MBI served only 16 of the 28 children and parents referred during FY 2020.
CFSA needs to find creative housing solutions to keep siblings together in foster care and to enable children to be placed with kin in foster care, guardianship or adoption.
According to the 2021 Needs Assessment, the Agency has only 50 licensed providers to care for three or more children in foster care. However, there are 194 foster children in a family of three or more siblings, which indicates the need for more foster parents with the capacity and willingness to take groups of three or more siblings. CFSA should look for creative, out-of-the box ideas tor increasing placements for sibling groups. For example, CFSA could seek a public-private partnership to create a community of homes for foster parents who take in large sibling groups, in the mode of SOS Children’s Villages in Illinois and Florida. Perhaps this could be included as part of a development plan for a parcel owned by the city.
CFSA also needs to be more creative and proactive in finding housing for relatives who want to take in children who have been removed from their families, temporarily or permanently. CFSA’s oversight responses state what we already know: “For DC-based kin, the ongoing lack of affordable housing in the District continues to impact the families’ ability and/or willingness to provide licensed kinship care.” And it’s not just kinship care but also permanency. I recently heard of a teenager being pressured to accept guardianship with a foster parent with whom she is not bonded, even though a relative is willing and available but has been unable to find suitable housing. This is unacceptable. As it did with Wayne Place for youths leaving foster care, CFSA should work with the private sector to create housing for relatives who are providing a home for children in foster care – housing like Plaza West, a building for grandparents raising children that was created without CFSA involvement. It is not acceptable to force children into guardianship with unrelated foster parents because relatives cannot find housing.
CFSA is not making sufficient efforts to ensure educational success for foster youth.
Education outcomes for District foster youth are truly horrendous. Foster youth aged 15-21 for whom Grade Point Average (GPA) information was available had a median GPA of 1.98 in the last academic year, according to the oversight responses. And only 68% of the foster youth who were eligible to graduate high school in June 2021 graduated or got a GED by that date. The blame for this abysmal school performance should not be placed entirely on CFSA: most of these children were probably struggling academically when they were removed from home. After all, many of these children came into foster care with a history of chronic absenteeism and school transfers. But if CFSA is going to remove children, it needs to take responsibility for improving their educational performance regardless of what it was before.
There are some things CFSA can do to improve educational performance among foster youth that have drawn little attention. For one, CFSA needs to make sure that foster parents are involved with the schools that the children in their custody attend. It is well-known that home-school communication is critical to school success. But when I was a social worker at a private agency working with Maryland foster parents of CFSA youth, many foster parents I worked with had never even been to the children’s schools, especially when these schools were in the District. They certainly did not attend Back to School Nights and parent-teacher conferences. Foster parents should be told that attendance at these events and regular communication with the schools is required. Secondly, CFSA needs to end the practice of pulling kids out of school for a whole day in order to attend one medical, dental, or court appointment. When I was working in the system, I found that family support workers usually made appointments during school hours because they were busy after school taking youths to family visits or therapy. For the same reason, they usually made these appointments in the middle of the day, ensuring the maximum loss of school time. Requiring foster parents to take children to these appointments might help solve this problem; it should clearly be their job anyway. These two steps, requiring foster parent involvement and stopping system-caused school absenteeism, would be a good place to start in improving foster children’s school performance. Monitoring the performance of the tutoring provider is another; I’ve heard too much over the years about incompetent tutors.
OYE Vocational specialists must be replaced.
The 2022 Needs Assessment states “CFSA has identified a gap for career preparation and available employment supports for youths.” That’s putting it mildly! In FY 2019 CFSA eliminated OYE’s Career Pathways unit and replaced it with the LifeSet program, which is not dedicated to career preparation or staffed with vocational specialists. There are no vocational training specialists at CFSA, only college specialists. As a result, there are NO youth currently enrolled in vocational training programs, according to the 2022 oversight responses. Around the country and here In the District there is a growing recognition that college is not for everyone, especially for those who are not likely to complete it. Many jobs requiring vocational training or apprenticeships provide a path into the middle class and a much better option than college for youths with poor academic skills. At this time of unprecedented labor shortages, it is a shame that the agency is not taking advantage of this opportunity to get our young people into good jobs. In the Needs Assessment CFSA indicates it is working with the Department of Employment Services to address this gap; the Committee should encourage the agency to address it with the urgency and intensity it deserves.
CFSA has neglected its responsibility get foster youth vaccinated
As I have written, CFSA seems to be prioritizing parental consent, even when not required by law, over the health of foster children and containment of Covid-19 in the District of Columbia. Moreover, it appears that the agency been reluctant to educate older foster youth about the benefits of vaccines. They don’t even know how many foster children have been vaccinated. And they have not reported how many have gotten Covid-19. This is not acceptable.
Conclusion: CFSA appears to have lost interest in its primary mission of protecting abused and neglect children.
In conclusion, CFSA continues to struggle to carry out its primary mandates of investigating allegations of abuse and neglect and responding appropriately with in-home supervision and support and foster care when necessary. Yet, despite these struggles, CFSA is eager to add more responsibilities to its plate. As the agency explains in its oversight responses, it wants to “transform from a child welfare system to a child and family well-being system.” This sounds great on first hearing but does not bear closer scrutiny. Child and family well-being are dependent on all the health, education and human services agencies in the District of Columbia. CFSA is having enough trouble accessing the services of these agencies for its current clients. Why not concentrate on performing its core duties rather than expanding them? I must acknowledge that CFSA is being encouraged on this misguided path by the federal Children’s Bureau, which has included the agency in its partnership to do exactly what CFSA is proposing. But just because it is being promulgated by the feds does not make it a wise policy.
The expansion into primary prevention through creation of the Family Success Centers is a prime example of this desire to broaden CFSA’s mission when the agency struggles to perform its core responsibilities adequately. Prevention of child maltreatment is not in the original mandate of child welfare agencies, and for good reason. If anything, child maltreatment prevention is normally conceptualized as a public health function, which is why home visiting programs are generally provided by health departments. More and more jurisdictions, including our neighbors in Maryland and specifically Baltimore, are investing in Family Connects, which provides a hospital visit from a nurse to every newborn to assess risk and refer to appropriate services. Family Connects has been shown by randomized controlled trials to reduce emergency room visits and hospital stays by 50% in the first year of life and CPS investigations by 44% in the first two years of life. The jurisdictions that have adopted Family Connects understand that neighborhood family support centers will never reach the most at-risk children, whose parents are too mentally ill, impaired by drugs, or overwhelmed to recognize that they need help.
I have some ideas about why CFSA (and the Children’s Bureau for that matter) appears to have lost interest in its core mandate of protecting children and providing a safe haven for those who must be removed from their homes. But until we figure out how to prevent child maltreatment, and even after we do, there will still be maltreated children who need to be protected. CFSA may have lost interest in these duties, but it is up to the Committee and the entire Council to remember our most vulnerable children and make sure the agency performs its core mandates.
CFSA’s Internal Child Fatality Report for 2020 was released on October 27, 2021. It provides information on 40 deaths of children and young adults whose families were known to CFSA within five years of their deaths. The report shows that most of these families had been reported to CFSA multiple times in the past five years. Many of them had experienced investigations and received CFSA services through in-home and foster care cases. Despite these interventions, these children had died within five years of CFSA’s ending its involvement. The report contains the lessons that CFSA drew from these deaths, but a careful reading suggests that the agency has not taken full advantage of this opportunity to improve future practice. Moreover, the report does not provide the information that interested readers need to make their own conclusions about agency practices and needed changes.
CFSA’s internal fatality report is different from the annual report of the citywide Child Fatality Review Team, which covers all deaths of young people up to age 18 and some deaths of those aged 19-21. The CFSA report focuses on fatalities of young people up to age 24 whose families were known to the agency within five years of their deaths. These fatalities are reviewed by the agency’s Internal Child Fatality Review (ICFR) Committee, and this report summarizes the results. As the report explains, the internal fatality review process “is one of CFSA’s strategies for examining and strengthening child protection. It provides the Agency with specific information that helps to address areas in need of improvement and to identify any systemic factors that require citywide attention - all with the goal of reducing preventable child deaths.”
The 2020 child fatality report includes only those child deaths that occurred during Calendar Year (CY) 2020 and were reviewed by the ICFR Committee during 2020 or in the first three months of CY 2021. An additional fifteen deaths that occurred in CY 2018 and CY 2019 but were reviewed in CY 2020 are summarized briefly in an appendix but are not included in the narrative and data charts provided in the body of the report. I discussed this timing issue in depth last year, when the report excluded half of the deaths reviewed during 2019. This year CFSA has improved the coverage of its report, at least in part by including cases reviewed up to March 31 of 2021: this report includes 40 (or 72 percent) of the 55 deaths reviewed between January 1, 2020 and March 31, 2021. But it is still hard to understand the purpose of leaving out more than a quarter of the deaths reviewed during the period covered by the report. All of these deaths took place in 2018 and 2019, not many years in the past. The report states that the ICFR Committee reviewed these earlier cases “as part of its internal continuous quality improvement (CQI) efforts,” but also that “[i]n line with CFSA’s CQI efforts and based on the known fatalities that occurred during CY 2020, ICFR Committee members made practice recommendations to potentially help reduce future child fatalities.” So it appears that the 15 fatalities from 2018 and 2019 were reviewed as part of CQI, but were not used to develop recommendations, which is the main purpose of CQI! Leaving out these cases accomplished nothing but giving the committee a smaller group of cases upon which to make recommendations and reducing the amount of information available to the public in the annual report.
Manner of Death
The manners of death* of the 40 children whose cases are included in the body of the report are displayed in the pie chart below. Half of these children were victims of “non-abuse homicide;” nine (or 22 percent) died of natural causes; five (or 12 percent) died in accidents; three (or seven percent) died because of abuse or neglect; and one died by suicide. The other two children’s manners of death were “undetermined” and “unknown.” While children who die from abuse and neglect after having previous contact with child welfare draw the most public concern, research shows that children who have prior contact with child welfare also tend to die more often from all causes than children with no such involvement, as I discussed in my post, Report of maltreatment: a major risk factor for child mortality.
Abuse and neglect homicides of children known to CFSA often draw public concern because the agency’s primary role is to protect children from abuse and neglect. But they are a small proportion of the deaths to children who were involved with CFSA in the past five years. Three, or seven percent of the deaths reviewed in this report, were abuse or neglect homicides. The ICFR Committee also reviewed one abuse or neglect homicide that occurred in 2018 or 2019 and is addressed only in the appendix to the report. We know nothing about this case, not even whether the death was caused by abuse or by neglect. The two abuse homicides that occurred in 2020 were young children who died by blunt force trauma. The information provided suggests that the 11-month-old was Makenzie Anderson. Shortly after Makenzie’s death Petula Dvorak reported in the Washington Post that other residents of the Quality Inn that was then serving as a shelter for homeless families knew that Makenzie was in danger. But CFSA refused to disclose whether anyone had reported their concerns to the hotline. This report tells us that somebody, sometime, did report their concerns about Makenzie’s family, but that is all it reveals.
Given what is publicly known, the other abuse homicide discussed in the report - a two-year-old African-American male who died from multiple blunt force injuries - was probably Gabriel Eason, who died on April 1, 2020. An autopsy showed old and new injuries to Gabriel’s body, including swelling of the head and brain, abrasions and contusions to the head and torso; lacerations of the kidney and liver; injuries to the heart and vena cava; cuts on the face and neck; blunt trauma to the genitals; and 36 rib fractures. We know that Gabriel’s childcare center called the CFSA hotline on October 9, 2019, six months before he died, but we do not know what action CFSA took or if there were other calls. Unfortunately this report does not tell us anything new.
The neglect homicide included in the report involved a seven-year-old African-American boy killed in a car accident. The child and his younger siblings were passengers in a car driven by their mother in a long drive back to the District from another jurisdiction. None of the children were in car seats and the mother had alcohol in her system. The mother was charged with first-degree vehicular homicide, seatbelt violations, and driving under the influence. She was taken into custody and the remaining children were placed with relatives. The report does not tell us when and how often CFSA received reports in this family or how the agency responded.
Gun Violence
By far the most common manner of death for fatalities reviewed in this report was “non-abuse homicide,” or homicide that was not the result of child abuse or neglect. Such “non-abuse homicides” were half of all deaths reviewed, and all 20 of these deaths were caused by gun violence. Unlike in cases of abuse homicide, the media rarely asks about the history of gun violence victims with CFSA. However, the connection between child welfare history and gun violence death became obvious to me as soon as I started sitting on the citywide Child Fatality Review Committee. I learned that many of the young victims of homicide grew up in families with long histories of reports to CFSA. Reports on one family often include allegations of physical abuse, positive toxicology of a newborn, lack of supervision, and extensive unexcused school absences. Many of these reports were unsubstantiated; others were confirmed but resulted in nothing but a referral for voluntary services; others resulted in the opening of in-home cases that eventually closed; and others resulted in children placed in foster care and later returned home. But the abuse and neglect continued. Many of these families fit the pattern of chronic child neglect, which occurs “when a caregiver repeatedly fails to meet a child’s basic physical, developmental, and/or emotional needs over time, establishing a pattern of harmful conditions that can have long-term negative consequences for health and well-being.” Many of these children, with little support at home, histories of trauma, and disconnected from school, find their companionship in the streets and take up violent and illegal activities. Of the male decedents reviewed in the 2020 CFSA report, four were known to have been involved with the juvenile justice system and two were known to be involved in criminal activity when they were killed.
Of course, not all of the children included in this report who died from gun violence came from abusive or neglectful homes or were involved in violence themselves. Some of them died because they lived in a neighborhood plagued by gun violence or were in the wrong place at the wrong time. The eleven-year-old mentioned in the report might have been Davon McNeal, who was caught in the crossfire of a gunfight. And Davon was probably not the only bystander among the 20 who died. But perhaps some of the other deaths could have been prevented with more aggressive CFSA action. For example, the agency could have offered better, more intensive and long-lasting services to the parents, with court supervision to ensure they were taken up. And crucially, the agency could have refused to give second, third, and fourth chances to parents who repeatedly failed to take advantage of these services.
Natural Causes: Nine fatalities, or 22 percent of the deaths included in the report, were due to natural causes. Three of these deaths were due to prematurity and another three were due to medical conditions at birth. One might think that these deaths could not have been prevented by CFSA action, but research suggests otherwise. A population-based study using data from 3.4 million births in California found that, controlling for baseline risk factors like low birthweight and preterm births, infants with more than one CPS report were more than three times more likely to die of medical causes than those without a CPS report. The researchers also found that among infants reported for maltreatment, periods of foster care placement reduced the risk of death from medical causes by roughly half. Unfortunately, as described by child welfare expert Dee Wilson, medically fragile children are often born to the parents that are worst equipped to care for them. Thus, some of these deaths might have been prevented with more aggressive interventions, including foster care, in earlier contacts with the agency.
Accidental Deaths/Unsafe Sleep: Five of the CY 2020 fatalities, or 13 percent, were deemed accidental. Unsafe sleeping arrangements were involved in four of these deaths. (The fourth was a 20-year-old riding a moped without a helmet). In total there were five fatalities related to unsafe sleep. The other one was classified as “undetermined.” On the citywide child fatality review panel, I have seen numerous cases of children dying in unsafe sleep environments in families with long histories of child welfare involvement, often for numerous children. We tend to focus on unsafe sleeping arrangements (such as bed sharing) as the cause of death, but the reality is much more complex. Almost invariably, the parents have used marijuana, alcohol or illegal substances before lying down with the baby, and they fail to wake up when the children are struggling to breathe. With unimpaired parents, these sleeping arrangements might not result in death. That is why another study found that adjusting for risk factors at birth (including low birth weight and late or absent prenatal care), the rate of Sudden Unexplained Infant Death (SUID) was more than three times greater among infants who had been previously reported for past maltreatment than among infants who had not been reported. And that’s why more intensive interventions (including foster care placement) with families that abuse substances might have prevented some of these deaths.
Suicide: The CFR Unit reviewed one death by suicide; incredibly the decedent was an 11-year-old girl who hanged herself from the shower rod in her home. One population-based study estimated that children with any CPS history were three times as likely to end their own lives than children without such a history, and an eleven year old taking her own life suggests that something must have been amiss in her family that the agency might have been able to observe. “The family received grief services,” according to the report. That is nice to know, but it would be more important to know what type of trauma could have caused the suicide of an eleven-year-old, and what CFSA knew and should have known about this family before the child took her own life.
Undetermined and unknown: One child’s cause of death was unknown because the child died outside of the District; that child was in foster care. One fatality was classified as undetermined because the autopsy findings were inconclusive. The decedent was two months old and was found unresponsive after being swaddled for about two hours in a motorized baby swing with a blanket propping up a pacifier so that it would stay in the infant’s mouth. Unsafe sleep practices may have contributed to the infant’s death, according to the CFR Unit. This case raises the same issues as the accidental deaths discussed above. Any family that would leave a two-month-old unsupervised in a swing for two hours with a propped bottle has severe parenting deficiencies beyond their knowledge of safe sleep practices-deficiencies that required aggressive intervention in order to protect the child.
Parents’ CFSA History as Caregivers
Nine of the 40 families reviewed in the report (or about 23 percent) were involved with CFSA at the time of the fatality. Of these nine families, five had an open foster care case, two had an open investigation, one had an open in-home case and an open investigation, and one had an open permanency case and an open CPS investigation. Obviously it is concerning that these fatalities could occur while CFSA was actively involved with the family. One has to wonder whether any red flags were disregarded. But without knowing the details of CFSA’s involvement with these families, it is impossible for readers of this report to make any conclusions about agency practice.
In addition to the nine families who had an open investigation or case at the time of the fatality, four families (10 percent) had a case or investigation closed within three months of the fatality, four families had a case or investigation closed within four to nine months of the fatality, and another four families had a closure within 10 to 12 months of the fatality. It is concerning that so many families had such recent contact with CFSA; one wonders whether the case closures were premature and whether any red flags were missed. One family was not included in these calculations because it had four referrals that were screened out and no investigations or cases. It is concerning that a family with a later fatality had four reports screened out and it would be interesting to know when those referrals came in and whether the CFR unit looked at why they were rejected. There has been some concern about the accuracy of hotline decision-making. In a 2016 study, conducted by the Center for the Study of Social Policy, the court monitor in the LaShawn class action suit, reviewers agreed with the decision to screen out the referral in only 73 percent of the 223 screened-out referrals studied.
The chart below shows the frequency of CFSA involvement for the families with fatalities. All of the families had more than one report to CPS within five years of the fatality, 31 families, or 77 percent of the families, had four or more reports. So these families were very troubled, and there were many opportunities for CFSA to intervene.
What happened as a result of these reports? All but two of the families had referrals that were screened out, with 40 percent having four or more such screened-out referrals. About 83 percent of the families had at least one investigation. Sixty-five of the families had between one and three family assessments, an alternative to traditional investigation that has been dropped by CFSA. Forty-three percent of the families had one or two in-home cases, and 33 percent had one or two permanency (foster care) cases. Again, this table shows that CFSA had many opportunities to assess and intervene with these families before their children died.
According to the table shown above, 33 families were the subject of investigations in the five years before the fatality. In Figure One of the report (not reproduced here) CFSA found that 19 families had at least one substantiated allegation in the five years before the fatality. That 33 of these families had investigations but only 19 (or about 58 percent) had at least one maltreatment finding suggests that many of these investigations may have failed to find existing abuse or neglect. Physical abuse was the type of allegation that had the largest number of substantiations (eight). Unfortunately, we do not know how many families received those eight substantiations; it could have been one family that received them all or several families could each have received a smaller number of substantiations. The other most frequent types of maltreatment substantiated were ‘failure to protect’ (five), and four each for inadequate supervision, substance use by parent or caregiver, unwilling/unable caregiver, positive toxicology of a newborn, educational neglect and exposure to domestic violence. It would also be valuable to see the number and subject of unsubstantiated allegations as well since a large body of literature documents the difficulty of accurately determining whether a child has been maltreated, which is why scholars often prefer to use referrals (rather than substantiations) as a metric for the rate of maltreatment.
It is no surprise that many families of children who died within five years of CFSA involvement had a long history of reports to child protective services. The known high risk level for children in a family that has multiple reports is the reason that CFSA requires a “Four-Plus staffing,” which is a special meeting for families with four or more allegations, when the last report occurred within 12 months. According to the report, these staffings “focus on gaps in practice or service delivery that may have contributed to a family returning to CFSA’s attention.” Among the 40 families included in the report, 15 met the qualifications for a Four-Plus staffing, and all of them received such a staffing. This result raises questions about the efficacy of these staffings in addressing families with multiple reports to CFSA.
CFSA’s Recommendations
Based on its fatality reviews, the ICFR Committee makes recommendations each year for CFSA and other District agencies for actions that might avert future fatalities. This year the committee made only three recommendations: provide support to child welfare professionals who experience traumatic stress; improve information sharing between DC government agencies, and encourage use of a comprehensive medical information platform among hospitals and medical providers in the District. The report explains that the last recommendation would address the problem of abusive parents who bring their children to different medical providers. It is possible that this recommendation was prompted by the case of Gabriel Eason, whose mother brought Gabriel to two different emergency rooms for his injuries, thus making it less likely that abuse would be suspected.
These are all good recommendations. But it is rather surprising that there are no recommendations to improve CFSA’s practice in conducting investigations and in-home and foster care cases. Given that nine of these decedents had an open investigation or case at the time they died, and another 12 had an open investigation or case within a year of the fatality, there is reason to wonder if anything could have been done differently in these cases. But without knowing the details of CFSA’s involvement with these families, it is impossible for reader of this report to make any conclusions about agency practice. The ICFR Committee was given the details on each case. Is it possible that they found no flaws in case practice that would lead to recommendations for the future? That is hard to imagine.
Even without being privy to case details, there are some potential recommendations that come to the mind of an educated reader. Given the fact that all 15 families that qualified for a Four-Plus staffing because of the extent of their history with CFSA actually had such a staffing, and a child died nevertheless, one might wonder if Four-Plus staffings are achieving their purpose. A reasonable recommendation might be to change these staffings or eliminate them entirely and replace them with something else. Given that among the allegations about the 40 decedents’ families by far the most allegations involved abuse, a potential recommendation might be that the agency heighten scrutiny for families that were reported for abuse. There is other evidence for such a proposal: one study found that children with a previous allegation of physical abuse sustained fatal injuries at 1.7 times the rate of children referred for neglect. Several years ago, the agency eliminated its Special Abuse Unit, which investigated allegations of physical and sexual abuse; one wonders if this was a step in the wrong direction.
Perhaps I am being too critical of CFSA’s internal child fatality report. It is difficult for an agency to criticize itself and recommend changes that may go against its ideological orientation. That is why some states give a Child Advocate, Ombudsperson or Inspector General the duty of investigating certain child fatalities in which the family was known to the child welfare agency. The City Council established the Children’s Ombudsperson in the 2020 legislative session and I advocated for that office to be given that responsibility. After putting that requirement in the original draft, the bill’s framers removed that provision. I hope the Council will consider amending the legislation to ensure that an impartial, independent party reviews some of these deaths and makes the reviews available to the public.
Reviewing the fatalities of children who were involved with CFSA in the five years preceding their deaths provides an opportunity for CFSA to suggest changes in its practices. However CFSA has not taken full advantage of this opportunity this year. First, by eliminating over a quarter of the cases it reviewed based on an arbitrary timeframe, the fatality review committee deprived itself of vital fodder for recommendations and withheld important information from the public. Second, the committee made no recommendations for changes in the agency’s investigative and case management practices that may have allowed serious red flags to be missed, leaving children vulnerable to serious maltreatment during or after their involvement with CFSA. Finally, the report represents a failure to inform the public about the performance of an agency that it pays for. Not only does CFSA’s 2020 internal fatality report fail to derive all the available lessons from CFSA’s mistakes but it does not provide the details necessary to enable members of the public to draw its own conclusions about agency performance. That’s why the City Council should give the new Children’s Ombudsperson the responsibility for investigating and reporting about such fatalities.
*”Manner of death” refers to the circumstances that caused the death, as opposed to “cause of death,” which refers to the specific disease or injury that led to the death
The Child and Family Services Agency (CFSA) has updated its Data Dashboard for the fourth quarter of the District of Columbia’s Fiscal Year (FY) 2021, which included July through September of 2021. As usual, hotline calls dropped with the closure of schools for the summer, and then rose again when school started in September. However there was no dramatic onslaught of referrals when students returned to in-person school compared to what happens in a typical September after summer vacation. Hotline workers screened out a smaller percentage of referrals in the fourth quarter than they did in the previous quarter, investigating a larger percentage of them but substantiating a somewhat smaller percentage of those they investigated. CFSA served a fairly constant number of children and families in their homes throughout the year. However, the foster care caseload has been dropping fast - with an 11.5 percent decrease from in the Fiscal Year ending September 30, 2021.
Referrals
Many experts have predicted that hotline calls (known as “referrals”) would skyrocket after children returned to school in person, and indeed this has happened in other jurisdictions around the country. In the District, referrals did begin increasing in the third quarter of FY 2020 and continued to increase in the two succeeding quarters, as shown in Table One, even though most children were still learning virtually. By the third quarter, there were 5,880 referrals, almost as many as the 6,058 referrals that came in the corresponding pre-pandemic quarter of 2019. The quarterly number of referrals fell drastically to only 2,997 in the fourth quarter (July through December 2021), which is a return to the seasonal pattern in which referrals drop in the summer, when school is out of session. The total number of referrals for the third quarter of 2021 (2,997) did not reach the level of the third quarter of FY 2019 (3,274), the last fiscal year before the pandemic. But fourth-quarter data hides the difference between summer vacation and school, which started on August 30 for DC Public Schools students.
As shown in Table One, referrals did rise in September 2021 to 1,148 from only 759 in August. That is considerably more than the 942 referrals in September 2020, but considerably less than the 1,377 calls in September 2019. The absolute difference in referrals between August and September of FY 2021 was smaller than in FY 2019 but the percentage difference was slightly greater. (FY 2020 showed less of an increase between August and September referrals in both number and percentage, showing the effects of the pandemic and virtual schooling.) But there was no dramatic onslaught of referrals in the wake of schools opening in person in September 2021, compared to a normal September. However, based on FY 2019 data, October brings more referrals than September, so we will see what the next quarter’s data show.
Table One
Referrals in August and September, FY 2019-FY 2020
Referrals
FY 2019
FY 2020
2021
August
946
718
759
September
1377
942
1148
Difference
431
224
389
Percent Change
31%
24%
34%
Source: CFSA Data Dashboard, and Child Welfare Monitor, previous posts
Figure Two shows the number of referrals made by each reporting source in Fiscal Years 2019, 2020 and 2021. This number, which had dropped from 17,960 in FY 2019 to 14,046 in 2020 with the onset of the pandemic, bounced back to 17,422 in FY 2021, almost the same number as in FY 2019. School and daycare personnel are traditionally the largest referral source, and they actually made substantially more reports in FY2021 than they did in the pre-pandemic fiscal year, 2019 - 8,482 compared to 7,704. They also made a higher percentage of all reports-48.7% compared to 42.9 percent in FY 2019. This increase in teacher reporting relative to FY 2019 may reflect teachers’ increased concerns about children missing too many days of online schooling last spring, as well as concerns raised by seeing children in the fall for the first time in 18 months.
Once a call comes into the hotline, it can be accepted as an “information and referral” to be referred to another agency; accepted for investigation; linked to an existing open investigation; or screened out as not requiring any response. Figures Three and Four show how as the number of referrals increased in the first three quarters of FY 2021, CFSA reduced the proportion it accepted. In an earlier post we suggested this might reflect the impact of CFSA’s belief that teachers make too many referrals for “compliance” purposes only. This belief led the agency to institute a new policy of rejecting educational neglect referrals for a family with whom the school or CFSA had been in contact within the previous 10 days of school. But in the fourth quarter, as referrals dropped after schools closed, CFSA screened out a smaller percentage of referrals. The agency screened out only 56.6 percent of referrals compared to the 75.0 percent screened out in the previous quarter. So the number of referrals accepted dropped much less than the total number of referrals received from 1124 in Quarter 3 to 1081 in Quarter 4.
Figure Five shows the large drop in the number of investigations in the first four pandemic quarters compared to four preceding quarters. In the fourth quarter of FY 2021, the number of investigations was closer to pre-pandemic levels but still lower - 1030 in FY 21 versus 1176 in FY 2019. Notably, the number of investigations hardly dropped in quarter 4 over quarter 3 even though the number of referrals (shown above) dropped greatly. This lack of a summer drop in investigations reflects the increased percentage of referrals accepted, as discussed above. It’s as if the agency was trying to keep the number of investigations constant by rejecting more referrals when they received more of them, but this may just reflect the lower credence given to referrals from schools.
An investigation can have several possible results. It can result in a finding of “inconclusive,” meaning the evidence is insufficient to prove maltreatment despite some indications it occurred; “unfounded,” which means “there was not sufficient evidence to conclude or suspect child maltreatment has occurred” “substantiated,” indicating that the evidence supports the allegation of maltreatment; “incomplete” (as defined in the CFSA Data Dashboard), or “child fatality,” which is defined as a “suspicious death of a child that may be due to abuse or neglect.” About 23 percent of investigations were substantiated in the most recent quarter, as shown in Figure Six. That was slightly lower than the 26 percent substantiated in the previous quarter. Figure Seven shows that number of substantiations fell in the summer quarter in accord with the smaller number of investigations and the lower substantiation rate.
When an abuse or neglect allegation is substantiated, several things may happen, depending on the assessed level of risk to the child or children in the home. The agency may take no action, refer the family to a community-based collaborative, open an in-home case, or place the child or children in foster care.
In-Home Services
When a CFSA investigator considers children in a family to be at high risk of maltreatment, but not in imminent danger, the policy is to open an in-home case for monitoring and services. Figure Eight shows the number of in-home cases opened by quarter, starting in the first quarter of FY 2020.* There were slightly fewer case openings in the summer quarter than the prior quarter, reflecting the decline in the number of substantiations. Figure Nine shows that the number of in-home case closures rebounded in Quarter 4 following a decline in the previous quarter. These may be random fluctuations or they may reflect unknown factors.
Table One shows that the total number of children being served in their homes was 1,290 on September 30, 2021, very slightly down from 1299 on September 30, 2020. That is not surprising, since the difference between entries to (119) and exits from in-home services (134) was very small as well.**
Table One
\Total Number of Children Served at Home and in Foster Care, FY 2020 and FY 2021
In-Home
In Foster Care
Total
Sept. 30, 2020
1299
694
1993
Sept. 30, 2021
1290
614
1904
Source: CFSA Data Dashboard, cfsadashboard.dc.gov
Foster Care
The number of children entering foster care decreased in the last quarter of FY 2021, after rebounding from a large pandemic-induced drop in the fall and winter quarters and then decreasing in the spring quarter. Fifty-nine children entered foster care in the last quarter of FY 2021, as shown in Figure Ten. Figure Eleven shows that exits from foster care decreased in Quarter 4 but were still more numerous than entries. There were 64 exits from foster care compared to 59 children entering care.
Figure Twelve shows the number and percentage of children exiting foster care for different reasons in FY 2020 and FY 2021. There were no big changes between the two years. In both years, reunification was the main reason for exits from foster care, though the percentage exiting through reunification decreased slightly from 41 percent to 39 percent, at the same time as the percentage exiting through adoption increased from 31 percent to 34 percent. CFSA does not post these data for earlier years, but perhaps this was due to a pandemic-induced suppression of adoptions in FY 2020. Smaller but still significant percentages left the system for guardianship (13 percent in 2020 and 12 percent in FY 2021) and emancipation (14 percent in FY 2020, declining to 12 percent in FY 2021), with very small numbers having died or entered the custody of another agency.
Figure Twelve
Children Exiting Foster Care by Reason for Exit, FY 2020 and FY 2021
Looking at the data for Fiscal Year 2021 in total, there were 251 entries into foster care and 327 exits in the four quarters ending on October 30, 2021. With exits eclipsing entries, the number of children in foster care should have fallen by approximately 76 children. And indeed, Table One above shows that the total number of children in foster care fell by 80 from 694 in September 2020 to 614 in September 2021.** This was a decrease of 11.5 percent, somewhat less than the 13.0 percent decrease between FY 2019 and FY 2020. The foster care rolls have been falling annually for years, but the decrease accelerated in Fiscal Year 2020, as shown in Figure Thirteen,*** and only slightly decelerated in FY 2021. When asked about the drop in the foster care rolls a year ago, CFSA responded that it reflects the agency’s continued commitment to keep families together without formal child welfare involvement when it is safe to do so.
The total number of children served in their homes and in foster care decreased from 1993 to 1904, a decrease of 4.47 percent from FY 2020 to FY 2021, as shown in Table One above. Data from earlier years is available from the Center for the Study of Social Policy for the calendar year only. Figure Fourteen shows the number of children served both in foster care and in their homes in the calendar years from 2010 to 2019 and in September of 2021. That total has been decreasing for the last two fiscal years.
In conclusion, the fourth quarter showed the normal drop in referrals with the closure of school for the summer. There was an increase in hotline calls when schools reopened in person last September, but not the overwhelming influx of calls that some had predicted with the re-opening of school buildings. The number of children and families with in-home cases stayed stable, but the foster care population continued to drop-resulting in a small decline in the number of children served by CFSA from September 2020 to September 2021. CFSA has attributed its declining foster care numbers to its continued commitment to keep families together without formal child welfare involvement when it is safe to do so. We can only hope that CFSA is fulfilling this commitment without jeopardizing child safety.
*These numbers include all in-home cases opened as a result of CPS investigations. It does not include a small number of cases opened as a result of case transfers from foster care or adoption units or in-home cases that are the result of reunifications and are managed by the foster care units.
**There is a small difference between the number of exits (134) minus entries (119) from in-home care and the year-to-year difference in the number of children in in-home care (9) and a similar small difference between the number of exits minus entries to foster care (76) and the year-to-year difference in the foster care caseload (80). The small anomalies reflects standard data entry delays when there is a change in a child’s status.
***The accelerated decrease in the foster care rolls did not seem to be related to the pandemic. When we compared data from March to September of 2019 and 2020, we found that 74 fewer children entered foster care and 68 fewer children exited it, suggesting that the pandemic had little effect on the total foster care caseload.
The COVID-19 vaccine has been approved for all children aged 12 and older and has been proven safe and effective. The Mayor has strongly encouraged all eligible youths to be vaccinated, organized special vaccination clinics in schools, and announced a variety of incentives for youth vaccinations. Children in foster care are wards of the District, and one might think that the agency would act as the Mayor has encouraged parents to do, and make vaccinating its wards the top priority. However, it appears that that for CFSA, vaccinating its youth falls somewhere below other priorities, such as protecting parents’ rights to refuse vaccinations for their children.
In the District of Columbia, all children aged eleven and up are allowed to consent to their own vaccinations under a new law, the Minor Consent for Vaccinations Amendment Act of 2020. However, in a new Administrative Issuance (AI) released on on July 22, CFSA takes pains to clarify that it has chosen not to take full advantage of this opportunity to get foster youth vaccinated. In the AI, titled “How to Obtain Informed Consent for COVID-19 Vaccination for Children Served in Out-of-Home Care,” CFSA states that “This law does not negate the Agency’s ability to first seek parental consent, rather, it provides an avenue for consent when a parent or caregiver does not consent.” The agency goes on to state that it has decided to continue obtaining parental consent for vaccination for youth 11-17 unless parental rights have been terminated. Youths aged 18-21, who are “developmentally capable,” are allowed to consent to their own vaccine.
Given that CFSA has decided to request consent from all parents of children under 18, the agency could have required social workers to ask all parents of children in their caseloads to consent to the COVID-19 vaccine for their eligible children by a certain date. But they did not do so. Instead, the AI states that “Social workers will ensure that parents receive the share (sic) “Fact Sheet for Recipients and Caregivers” before obtaining their consent to ensure they are making an informed decision about their child receiving the COVID-19 vaccine.” Thus, the focus is on ensuring that social workers share the fact sheet if they request consent, rather than requiring that they ask all parents to consent to the vaccination for their children. Moreover, there is no requirements that these conversations be documented so that the agency can determine how many parents have been asked and how many have agreed; documentation is required only when parents “refuse or are unable to provide consent.”
We do not know how proactive the agency is being in requesting parental consent for children aged 12-17 to receive the COVID-19 vaccination. According to Kera Tyler, CFSA’s Communications Director, “our social workers are actively encouraging parental consent for the vaccine for children in care over the age of 11. By sharing relevant educational materials along with District incentives, our Parent Engagement Education and Resource (PEER), family support workers, and social workers are facilitating conversations with both birth and resource parents to support vaccination for youth 12 and older.” The emphasis on educating parents and using peer support workers is laudable. But with no record of how many parents are being reached with such communication and what the results were, there is no way to know how successful these efforts have been.
The AI does provide a procedure for a child aged 17 or under who wants to get vaccinated to consent to the vaccine if the agency has not obtained parental consent for whatever reason. In such a case, “CFSA will ensure that the child meets with their primary care provider,” according to the AI. The social worker must “ensure that age and developmentally appropriate information about the COVID-19 vaccine is provided to the child by the primary care provider…The primary care provider must confirm that the child understands that they are making an informed decision about their consent to receive the vaccine.” And If the child does consent to the vaccine, “the primary care provider will be responsible for arranging and administering, recommending, or prescribing the vaccine.”
This is a rather cumbersome procedure. The extra step of seeing the primary care provider is not required of other District children consenting to their own vaccinations. Arranging and carrying out this visit is a burden for already taxed social workers. It is not even clear that primary care providers are willing to schedule such appointments. In any case, following this procedure is sure to delay vaccination. Perhaps most importantly, this provision makes it harder for young people in foster care than for their peers who are not in foster care to consent to their own vaccinations. One has to wonder if any children have been vaccinated under this provision, but CFSA has not been collecting vaccination data, as discussed below.
The situation is different for foster youth aged 18 to 21. According to the AI, these young people can consent to vaccinations unless they have a mental disability. The AI states that “Social workers will ensure that youth receive the share (sic) “Fact Sheet for Recipients and Caregivers” before obtaining their consent to ensure they are making an informed decision about receiving the COVID-19 vaccine.” Again, the instructions are more about ensuring that social workers share the fact sheet if they do request consent, rather than requiring that they make this request of all youth in this age category. And without a documentation requirement, we have no idea about how often these conversations are being held and what the results have been.
As with parents, CFSA cannot document how proactive it is being in requesting consent for vaccination from older youth in foster care. According to Tyler, “For our older youth, CFSA social workers have distributed educational materials to youth on their caseloads, coordinated appointments, arranged transportation to and from vaccination sites, and promoted the District’s incentives as applicable.” I mentor a nineteen-year-old in foster care who was eligible early for the vaccine early based on medical status, and it was I who provided information about the vaccine, helped her obtain her appointments and drove her to both. She reported that her social worker “mentioned” the vaccine, but there was no offer of assistance in getting vaccinated.
Given the procedures restricting vaccine uptake among CFSA children aged 12 to 17 and the lack of guidance about vaccine among older youth, it is important to know how many youths in CFSA care have been vaccinated. Unfortunately, the agency is not collecting this information. This makes it impossible to know how successful their attempts at obtaining consent have been. CFSA is collecting reports of children who receive a positive diagnosis of COVID-19 but given that these diagnoses are medical data, Tyler states that CFSA is developing some quality control standards before making those figures public.
It is perhaps not surprising that CFSA is sensitive to the beliefs of parents and older youths about COVID vaccines. Most foster youths are Black and vaccine hesitancy is high in the Black community. This hesitancy and the misinformation on which it is based is indeed the biggest barrier to getting older youths vaccinated, according to the Chairperson of the Board of Directors of FAPAC, an organization representing foster parents in DC. It makes sense to focus on sharing educational materials along with incentives to encourage vaccination among foster youth.
But the health of our foster youth, foster parents, and the District of Columbia population overall should be the top priority during this critical time, and CFSA should spare no effort in ensuring that all youth get the necessary information, and that all who are ready to be vaccinated can get the vaccine without delay. We know that foster youths have more health problems than their peers who are not in foster care, some of which put them at high risk if they develop COVID-19. Children’s National Medical Center has reported a “dramatic increase” in pediatric COVID-19 cases over the summer, fueled by the Delta variant. Nationally, cases in children have reached the highest level since the start of the pandemic-more than a quarter of all new weekly cases.
There were 624 children in foster care in the District of Columbia as of June 30, 2021. More than half of these are 12 and older.* This is a small number relative to the total number of children in the District, but these children are under the District’s direct care. The Mayor has made vaccinations a priority for all eligible groups. One might hope that the District would set an example by making vaccination of its wards a top priority.
*According to the CFSA Data Dashboard, 47 percent of CFSA youth were aged 13 to 21 in the third quarter ending June 30; therefore it is likely that at least half of these youth were aged 12 to 21.